Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2014) Volume 4, Issue 2
Objective: Angiotensin II receptor blocker (ARB) has become first-line agent for the treatment of hypertensive patients because they are associated with an excellent effect for blood pressure control and a lower rate of occurrence of adverse reactions. To our knowledge, there is no report of the large-scale study that measures biomarkers in 1000 or more patients for long follow-up period. To compare the effects of ARB therapy and that of standard therapy except ARB on the changes of biomarker levels and the incidence of cardiovascular events, a trial of telmisartan prevention of cardiovascular diseases (ATTEMPT-CVD) was planned. Urinary albumin creatinine rates, plasma brain natriuretic peptide, serum high sensitivity c-reactive protein, urinary 8-hydroxy-deoxy-guanosine,
serum adiponectin, and high-molecular weight adiponectin were selected as biomarkers. These biomarkers are known to be predictive factors for cardiovascular event, renal dysfunction, or atherosclerosis.
Methods: ATTEMPT-CVD is a multicenter, prospective, randomized open-label, controlled trial with blinded endpoint assessment. High-risk patients with heart, peripheral, renal, or cerebrovascular disease or diabetes are being recruited and followed for 3 years. The randomization is performed as stratified randomization after age, gender, past history of disease and usage of angiotensin converting enzyme inhibitor are adjusted for. The biomarker assessment is performed at the start of the study (at registration), after 6, 12, 24 and 36 months from the start of the study. Furthermore, survey of general laboratory tests, cardiovascular events, adverse events, and drug compliance is also performed at the same point of biomarker assessment and after 3 months from the start of the study.
Conclusions: The ATTEMPT-CVD is the first large clinical trial focusing of the efficacy of ARB therapy on the relationship between prevention of cardiovascular event and the changes of biomarkers. This study will provide a novel insight into the significance of biomarkers considering the therapy on high-risk hypertensive patients.
Keywords: Angiotensin II receptor blocker; Biomarker; Cardiovascular event; Hypertension; Urinary albumin creatinine rates; Brain natriuretic peptide; High sensitivity c-reactive protein; Urinary 8-hydroxy-deoxy-guanosine; Adiponectin; Estimated glomerular filtration rate
Angiotensin Converting Enzyme (ACE) inhibitors reduce rates of heart failure, myocardial infarction, stroke, and death among patients with heart failure [1], left ventricular dysfunction [2-4], previous vascular disease alone [5-7], or high-risk diabetes [8]. ACE inhibitors reduce bradykinin degradation, which enhances vasodilatation, but increase the rates of angioedema and cough. The effect of Angiotensin II Receptor Blocker [ARB] on BP is the same as those of other antihypertensive agents, including Ca antagonists, ACE inhibitors, and others [9,10]. ARBs have become first-line agents for the treatment of hypertensive patients because they are associated with a lower rate of occurrence of adverse reactions than ACEIs and Ca antagonists. The ongoing telmisartan alone and in combination with ramipril global end-point trial (ONTARGET) demonstrated no inferiority of termisartan to ACE inhibitor ramipril with regard to death from cardiovascular causes, myocardial infarction, stroke, or hospitalization for heart failure in high-risk patients who had cardiovascular disease or diabetes mellitus but did not have heart failure [11].
Urinary albumin and blood Brain Natriuretic Pepetide (BNP) are biomarkers that are expected to improve by ARB administration [12-14]. There is also a report that urinary albumin and BNP were not improved by ARB [15]. Increased Urinary Albumin Creatinine Rates (UACR) have been linked to the development of diabetic nephropathy and macrovascular disease in patients with type 1 and type 2 diabetes [16,17]. In the Heart Outcome Prevention Evaluation (HOPE) sub-study, microalbuminuria increased the risk of cardiovascular events, absolute lethal and hospitalization due to congestive heart failure and regardless of the presence or absence of diabetes, microalbuminuria increased cardiovascular events [18].
Elevated plasma natriuretic peptide levels has also been reported to predict the risk of death and cardiovascular events after adjustment for traditional risk factors [19,20]. Although there are many studies that observed the relationship between the cardiovascular events and biomarker levels on enrolment, there is no report of the large-scale study that measures biomarker in 1000 or more patients in the time course.
In the present study, we will compare the effects of ARB therapy and that of standard therapy except ARB on the changes of biomarker levels. The effect of the two treatments on the incidence of cardiovascular events will be also compared. Moreover, the relationship between the incidence of cardiovascular events and the changes of biomarkers will be exploratorily reviewed.
A trial of telmisartan prevention of cardiovascular diseases (ATTEMPT-CVD) is a multicenter, prospective, randomized open-label, controlled trial with blinded end-point assessment. Patient enrollment started July 2009 and was completed in April 2011; each patient is followed up for three years. Patients are followed up at 168 institutions throughout Japan.
Study population
The inclusion criteria are outpatients, 40 = age < 80 years old, patients whose two latest casual blood pressure levels measured in the sitting position are = 140 mmHg (systolic blood pressure) or = 90 mmHg (diastolic blood pressure) or patients still need to lower their blood pressure even in patients with systolic blood pressure<140 mmHg and diastolic blood pressure<90 mmHg, ability to provide informed consent, and patients having at least one risk among the cardiovascular risks shown in Table 1. Blood pressure is measured at least twice at intervals of 1 to 2 minutes and if these two values largely differ, it is measured one more time; patients’ blood pressure levels are judged based on the mean value of the two closest blood pressure measurements. The exclusion criteria is type 1 diabetes, severe renal disorder (serum creatinine level = 2.0 mg/dL), heart failure (NYHA Classification III or IV), myocardial infarction, percutaneous revascularization and bypass grafting of coronary artery/lower extremity vessel, cerebral infarction, cerebral hemorrhage, subarachnoid hemorrhage and transient cerebral ischemic attack within 6 months before the observation period, malignant hypertension, secondary hypertension, pregnant women, clinically problematic allergic disease or past history of hypersensitivity to the drugs used, past history of significant adverse drug reactions, extremely poor biliary secretion or serious hepatic disorder, patients who require treatment for a malignant tumor, and other patients who are judged by the physician to be unsuitable for the study. Malignant hypertension is defined as the state of abnormally high blood pressure and occurring acute disorders in the target organ such as brain, heart, kidney, and great vessels.
| Diabetic factor | Type 2 Diabetes |
|---|---|
| Renal factors | Serum creatinine level for men should be 1.2 mg/dl to <2.0 mg/dl and for women 1.0 mg/dl to <2.0 mg/dl |
| Protein urea: qualitative value ≥+1 Protein urea: quantitative value: proteinurea corrected for urinary creatinine of ≥ 0.3g/g.creatinine in spot urine |
|
| Chronic kidney disease stage 3 or higher | |
| Cardiac factors | Past history of myocardial infarction at least 6 months prior to obtaining the informed consent Angina pectoris |
| Heart failure (NYHA Classification I or II) | |
| Left ventricular hypertrophy (thickness of the posterior wall of left ventricle ≥12 mm on echocardiography before obtaining the informed consent or Sv1 + Rv5 ≥35 mm on electrocardiography.) | |
| Transient or persistent atrial fibrillation | |
| Cerebral factors | Past history of cerebral infarction, cerebral hemorrhage, subarachnoid hemorrhage and transient cerebral ischemic attack at least 6 months prior to obtaining the informed consent |
| Peripheral artery factors | Past history of lower extremities bypass surgery or angioplasty at least 6 months prior to obtaining the informed consent |
| Ankle-brachial index of <0.9 or with intermittent claudication |
Table 1: Cardiovascular risks.
Study protocol
The study protocol is in agreement with the guidelines of the ethics committees at our institutions and the study complies with the Declaration of Helsinki. The institutional review board at each participating hospital approved this trial, and written informed consent was obtained from each patient.
Registration and allocation
If possible, the physician is requested to stop ARB for two weeks or more before registration when the physicians in charge at the study sites register the patient who has taken ARB. After patients are judged to be eligible as a subject during the observation period, the physicians in charge at the study sites send the case registration form to the independent allocation center for the patient's enrollment. The independent allocation center receives the patients’ information by fax from the physicians. The patients are allocated to either the ARB group or the non-ARB (standard treatment except ARB) group. The randomization is performed as stratified randomization after age = 65 or age<65, men or women, past history of cardiovascular events, past history of diabetes mellitus, and usage of ACE inhibitor are adjusted (Table 2).
| Gender: Male or Female Age: <65 years old or ≥65 years old Past history of cardiovascular diseases: Yes or No Complication of diabetes: Yes or No Concomitant use of ACE-I: Yes or No |
| ACE-I=angiotensin converting enzyme inhibitor |
Table 2: Allocation factors.
The independent allocation center faxes back to the physicians in charge at the study sites after the allocation and notified the physicians the treatment group to which the patient is allocate within 30 minutes from the fax receiving.
Study drugs
Telmisartan is used for the patients allocated for the ARB group. On the other hand, standard treatment except ARB is performed for the patients allocated for the Non-ARB group.
Start of the study
After completion of registration and allocation, administration of telmisartan at the indicated low (20 mg) or middle (40 mg) dose is started in the ARB group. Or, additional antihypertensive drug except ABR is started in the Non-ARB group. The dose level is selected depending on the patient's condition. The dose level of telmisartan is increased to the middle or the highest dose (80 mg) (daily dose) for patients who do not achieve the target blood pressure. In this regard, however, the dose increase is eventually left to the discretion of the physician because the patient's condition needs to be considered. The rough standard is as described in Figure 1.
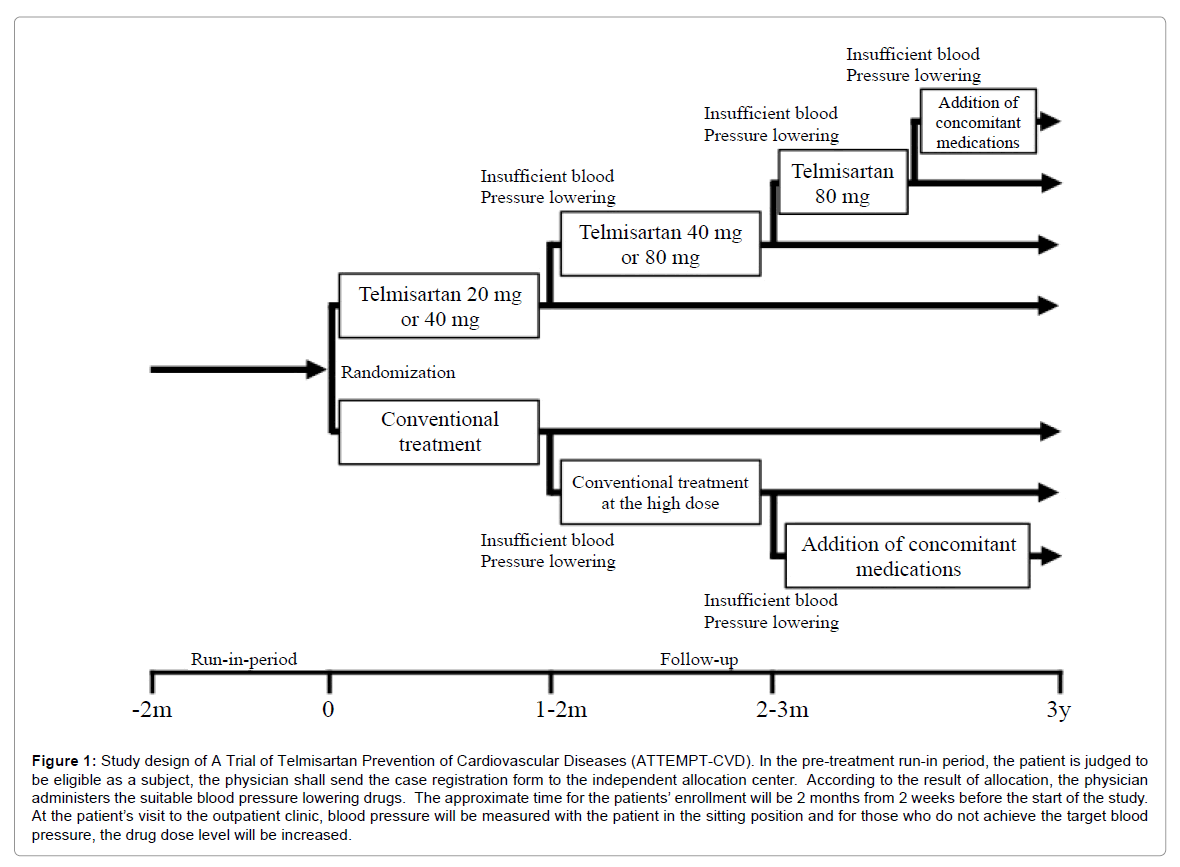
Figure 1: Study design of A Trial of Telmisartan Prevention of Cardiovascular Diseases (ATTEMPT-CVD). In the pre-treatment run-in period, the patient is judged to be eligible as a subject, the physician shall send the case registration form to the independent allocation center. According to the result of allocation, the physician administers the suitable blood pressure lowering drugs. The approximate time for the patients’ enrollment will be 2 months from 2 weeks before the start of the study. At the patient’s visit to the outpatient clinic, blood pressure will be measured with the patient in the sitting position and for those who do not achieve the target blood pressure, the drug dose level will be increased.
Survey
The physicians examine the survey items at the start of the study (at registration), after 3, 6, 12, 24 and 36 months from the start of the study, at a discontinuation/dropout, at the occurrence of any cardiovascular event, and at the occurrence of any adverse event. Thereafter, the physicians in charge at the study sites describe the results of the survey in the required forms and send them to the independent data center.
Survey at the start of the study (at registration)
Inquiry
Gender, date of birth, time when the patient is diagnosed with hypertension, complications (past or present history of cardiovascular diseases, presence or absence of diabetes, other complications), drugs used (antihypertensive agents, medicine for diabetes, hypolipidemic agents, antithrombogenic agents), history of alcohol consumption and smoking history are inquired.
Physical findings
Height, body weight, abdominal circumference, blood pressure and the pulse rate are measured.
Laboratory tests
Blood cell count, general blood biochemistry (AST, ALT, LDH, creatinine, estimated glomerular filtration rate (eGFR), urea nitrogen, uric acid, Na, K, Cl, total cholesterol, LDL cholesterol, HDL cholesterol, total protein, albumin, triglycerides, blood glucose, HbA1c), urine test (sugar, protein (quantitative, qualitative), creatinine, occult blood, special test (UACR, plasma BNP, serum high sensitivity c-reactive protein (hsCRP), urinary 8-hydroxy-deoxy-guanosine (8-OHdG), serum adiponectin, high-molecular weight adiponectin), standard 12-lead ECG, and chest X-ray are examined.
Survey 3 months after the start of the study
Drug compliance, concomitant drugs and concurrent therapies, blood pressure and pulse rate, subjective symptoms and objective findings, occurrence of cardiovascular events, occurrence of adverse events, and discontinuation/dropout are surveyed.
Survey at 6, 12, 24 and 36 months after the start of the study
Drug compliance, concomitant drugs and concurrent therapies, blood pressure and pulse rate, and abdominal circumference (only at 36 months after the start of the study), subjective symptoms and objective findings, general laboratory tests, annually standard 12-lead ECG, annually chest X-ray examination (time is not specified.), occurrence of cardiovascular events, occurrence of adverse events, and discontinuation/dropout are surveyed.
Patients are followed up at each hospital visit or by telephone if necessary. Follow-up visits are scheduled every 2 weeks for patients seen in a clinic setting and every 4 weeks for patients seen in a hospital setting. Data for patients who are lost to follow-up are included at the day of last follow-up.
Discontinuation and dropout
In case the physicians in charge judge that continuation of the study is difficult due to discontinuation of administration of the study drug, patients' withdrawal of informed consent, or impossible follow-up etc., the physicians in charge discontinue the study and send a discontinuation/dropout report to the independent data center. In case a patient does not visit the institution for 3 months or longer, the patient's condition is confirmed by phone or mail, etc.
Cardiovascular events and adverse events
The cardiovascular events consist of cerebral events, coronary events, cardiac events, aortic/peripheral arterial events, complication of diabetes, and aggravation of renal function. The detail of each cardiovascular event is shown in the Table 3. Adverse events refer to all unfavorable signs, symptoms or diseases occurring during the study period regardless of the causal relationship with the study drug. All cardiovascular events are adjudicated by the independent Events Monitoring Committee that is unaware of the group assignments. All adverse events are also adjudicated by the independent Data and Safety Monitoring Committee. The Data and Safety Monitoring Committee monitors the safety and efficacy of the study during the study period.
| Name of events | Applicable events |
|---|---|
| Cerebral events | Stroke (cerebral infarction, cerebral hemorrhage, subarachnoid hemorrhage, unknown type of stroke), transient ischemic attack |
| Coronary events | Myocardial infarction, angina pectoris, asymptomatic myocardial ischemia |
| Cardiac events | Myocardial infarction, angina pectoris, asymptomatic myocardial ischemia, heart failure |
| Aortic/peripheral arterial events | Aortic aneurysm, aortic dissection, arteriosclerotic disease (aorta, carotid artery, renal artery, mesenteric artery, peripheral artery, etc.) |
| Complications of diabetes | Diabetic nephropathy*, diabetic retinopathy*, diabetic neuropathy* |
| Aggravation of renal function | Doubling of serum creatinine level, ESRD (initiation of dialysis, renal transplantation) |
Table 3: Detail of cardiovascular events.
Endpoints
Primary endpoint is longitudinal data of UACR and plasma BNP in each treatment group (the change from baseline and their percent change). Secondary endpoint was longitudinal data of urinary 8-OHdG, serum adiponectin, high-molecular weight adiponectin, serum hsCRP, eGFR in each treatment group (the change from baseline). Moreover, secondary endpoints are difference in biomarkers (before-and-after comparison and inter-group comparison at each measurement time point and at the final measurement time point), time until occurrence of an event, and relationship between incidence of cardiovascular events and the 7 biomarkers.
The primary endpoint of this research is the change in UACR and plasma BNP from baseline values, and in statistical analysis, inter-group comparison by closed testing procedure is planned for the respective markers. The sample size necessary to assess the effect of the test drug on UACR and plasma BNP was calculated. As a result, the sample size necessary for the research was confirmed to follow the sample size necessary for verification in plasma BNP.
Based on a comparison between ramipril and telmisartan, plasma BNP level decreased from baseline by 2.6pg/mL in the ramipril group and by 7.0 pg/mL in the telmisartan group after 3 months of treatment [21]. When these values are applied to a repeated measurement model with a level of significance of 0.05, power of 0.80, the 3 observation points and a correlation coefficient between respective observation points of 0.7 [22], the necessary sample size of each group turns out to be 450 cases. This result indicates that the difference in plasma BNP level would be larger by about 3.8pg/mL in the telmisartan group than in the ramipril group after 3 months of treatment. As described above, in case the level of significance was set at 0.05, the power at 0.80 and the standard deviation in both groups at 20, 435 cases would be required for each group (two-sample t-test).
As for UACR, a comparison with the ARB valsartan showed that UACR decreased by 32.7% from 28.1 mg/g to 18.9 mg/g in the telmisartan group [23]. While in the group administered the ACE inhibitor ramipril, UACR decreased by 4.2% from 14.4mg/mol to 13.8mg/mol after 3 months of treatment [24]. When the results described above are applied to the already described repeated measurement model and the comparison involves 500 cases per group with the level of significance set at 0.05, the number of observations is 3 and the correlation coefficient between the respective observation time points is 0.7, the power exceeds 0.9. Therefore, the rationale for setting the sample size for plasma BNP can also serve for UACR.
As efficacy analysis population, a Full Analysis Set (FAS) and a Per Protocol Set (PPS) were defined. The primary efficacy analysis population will be FAS, an analysis identical to that carried out in FAS will be carried out in PPS and consistency of the results will be reviewed. The FAS shall be composed of the remaining patients after the patients who are not done blood sampling for biomarkers are excluded from the allocated patients. The PPS shall be composed of the remaining patients after the patients shown in the Table 4 are excluded from the FAS.
| Ineligible patients |
|---|
| Patientswho withdraw their consent |
| Patientsfor whom the initial blood sample is collected later than 2 weeks from the start of administration of the study drug |
| Patientswho start taking the study drug later than 3 months from the initial blood collection at the start of the study or patients who do not start taking the study drug |
| Patients who discontinue taking the ARB within 1 week before the start of the study |
| Patientswho are administered any prohibited drug for 1 month or longer |
| Patientswho take <80% of the study drug |
| Patientswho do not take the study drug is 1 month or longer |
Table 4: Exclusion criteria for per protocol set.
Safety analysis population shall be composed of the subjects who receive at least one dose of the study drug and whose safety information is obtained. In this regard, however, the subjects who withdraw their consent will be excluded.
The summary statistics shown in this document refer to the sample size, mean value, standard deviation, and minimum value, median and maximum value. Clopper-Pearson method will be used to calculate the confidence interval of proportion. In contingency table analysis, Fisher's exact test will be used for 2 × 2 table (two by two table) and χ2 test will be used for other items. Yates’ correction will not be implemented. The software to be used in this statistical analysis will be Windows SAS Version 9.2 or subsequent versions. P-values of less than 0.05 were considered statistically significant.
Primary endpoints
Based on the change from baseline of the biomarkers (UACR, plasma BNP) and their percent change, the profile will be compared between the treatment groups and reviewed by repeated-measure analysis of variance with measurement time points as repetition. Primary endpoints will be analyzed by the closed testing procedure in the order of UACR, plasma BNP, and their percent change in consideration of multiplicity.
Secondary endpoints
Relationship between the treatment groups and longitudinal data of biomarkers (the change from baseline)
Based on the change from baseline of the biomarkers (urinary 8-OHdG, serum adiponectin, high-molecular weight adiponectin, serum hsCRP, eGFR), the profile will be compared between the treatment groups and reviewed by repeated-measure analysis of variance with measurement time points as repetition.
Change of biomarkers at each measurement time point and at the final measurement time point
Summary statistics will be calculated for observed values at each measurement time point and change from baseline to each measurement time point and to the final measurement time point by group.
Comparison will be implemented for values at each measurement time point and at the final measurement time point will be compared with those at baseline by paired t-test. Change at each measurement time point and at the final measurement time point will be compared between the two groups by analysis of covariance with the baseline value as covariate. As these reviews will be exploratorily, multiplicity will not be adjusted. Concerning UACR and eGFR, the correlation coefficient will be obtained for the observed value at baseline and change from baseline at each measurement time point.
Time until occurrence of an event
For the following cardiovascular composite events (A) to (D), Kaplan-Meier curves will be prepared and time until occurrence of an event (median) and its 95% confidence interval will be obtained. Groups will be compared using log-rank test with the treatment group as a factor. Using Cox proportional hazard model, the hazard ratio of the ARB group to the Non-ARB group and its 95% confidence interval will be calculated.
(A) Occurrence of fatal and nonfatal composite cardiovascular events (cerebral events, cardiac events, aortic/peripheral arterial events, complications of diabetes, aggravation of renal function) shown in Table 3.
(B) Death from events other than cardiovascular events (non-cardiovascular death)
(C) Occurrence of composite cardiovascular events and non-cardiovascular death
(D) Occurrence of cardiac events and vascular events (cerebral events, cardiac events, aortic/peripheral arterial events)
Concerning subgroups, the same analysis will be carried out in subgroups of gender, age (<65 years old, = 65 years old), past history of cardiovascular diseases, complication of diabetes, concomitant use or not of ACE-I, eGFR (<60, =60 mL/min/1.73 m2), UACR (<30 mg/gCr, =30 mg/gCr), and BMI (<25 kg/m2, =25 kg/m2).
Relationship between occurrence of cardiovascular events and various biomarkers
As for the relationship between the biomarkers (UACR and plasma BNP, urinary 8-OHdG, serum adiponectin, high-molecular weight adiponectin, serum hsCRP) and occurrence of cardiovascular events, the following will be exploratorily analyzed.
Relationship between biomarker values and occurrence of cardiovascular events
For presence or absence of occurrence of cardiovascular events, logistic regression analysis will be carried out for the conventional risk factors shown in Table 5. Variables will be selected by step-down procedure.
| Items | Handling |
|---|---|
| Gender | Male/Female |
| Age (at of the time informed consent was obtained) | <65 years old / ≥65 years old |
| Body mass index | <25 kg/m2 / ≥25 kg/cm2 |
| Smoking history | Smoker/Ex-Smoker/Non-smokeer |
| Diabetes | Yes/No |
| Hyperlipidemia | Yes/No |
| eGFR | <60 mL/min/1.73 m2/ ≥60 mL/min/1.73 m2 |
| Past history of cardiovascular diseases | Yes/No |
Table 5: Conventional risk factors.
Any baseline value of a biomarker, value of a biomarker at the final measurement time point (the latest observed value before occurrence of an event, observed value at the final measurement time point in patients who do not develop an event) and change in biomarker (change from the baseline value to the value at the final measurement time point) will be added to the conventional risk factors and the same review will be implemented.
Calculation of C-statistics and net reclassification index
For observed values of the biomarkers (UACR and plasma BNP, urinary 8-OHdG, serum adiponectin, high-molecular weight adiponectin, serum hsCRP, eGFR), usefulness as a prediction model of risk factors for occurrence of cardiovascular events will be evaluated. Prediction of occurrence of events by conventional risk factors (Framingham Heart Study: coronary heart disease, 2-year risk) and prediction model in combination with the biomarkers will be compared and evaluated using C-statistics [25] and net reclassification index (NRI) [26].
Trial progress and baseline characteristics of the patients
As shown in Figure 2, the study screened 1267 patients from July 2009 to April 2012. Twenty-two patients met exclusion criteria. We randomly assigned 1245 patients, however, 17 patients were not done blood sampling for biomarker measurement. Finally, the study was started as follow: 615 patients in the ARB group and 613 patients in the Non-ARB group. Tables 6 and 7 summarized the characteristics of the patients at baseline. There was no significant deference in the baseline characteristics between the ARB and Non-ARB groups as shown in the Table 6.
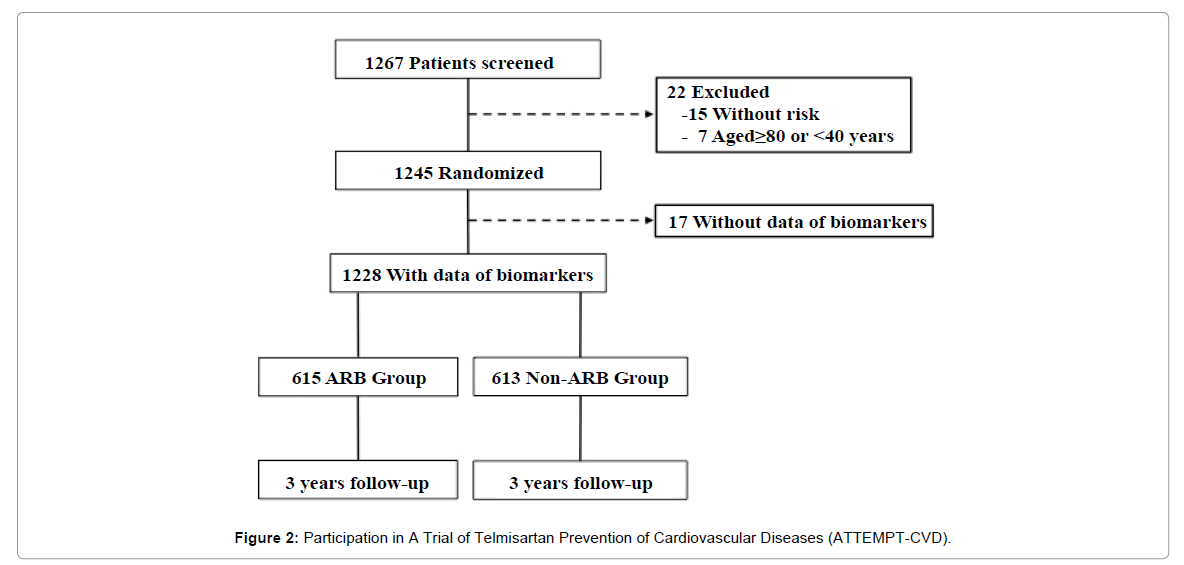
Figure 2: Participation in A Trial of Telmisartan Prevention of Cardiovascular Diseases (ATTEMPT-CVD).
| Total No (%) or mean ± SD | ARB Group No (%) or mean ± SD | Non-ARB Group No (%) or mean ± SD | |
|---|---|---|---|
| No. of patients | 1228 | 615 | 613 |
| Men, (%) | 715 (58.2) | 359 (58.4) | 356 (58.1) |
| Age, years | 66 ± 9 | 66 ± 9 | 66 ± 10 |
| Body mass index, kg/m2 | **25 ± 4 | ##25 ± 4 | &25 ± 4 |
| Systolic blood pressure, mmHg | 150 ± 16 | 151 ± 16 | 150 ± 15 |
| Diastolic blood pressure, mmHg | 84 ± 12 | 85 ± 12 | 84 ± 12 |
| Pulse rate, beats/min | 72 ± 11 | 72 ± 11 | 73 ± 11 |
| Current smoker, (%) | *216 (17.7) | #107 (17.5) | &109 (17.9) |
| Past smoker, (%) | *263 (21.5) | #133 (21.7) | &130 (21.3) |
| Every day alcohol use, (%) | *308 (25.2) | #157 (25.7) | &151 (24.8) |
| Sometimes alcohol use, (%) | *313 (25.6) | #156 (25.5) | &157 (25.7) |
| Dyslipidemia, (%) | *704 (57.6) | #352 (57.5) | &352 (57.7) |
| Angiotensin converting enzyme inhibitor combined use, (%) | 72 (5.9) | 35 (5.7) | 37 (6.0) |
| Estimated glomerular filtration rate, mL/min/1.73 m2 | *72.7 ± 19.7 | #72.4 ± 19.6 | &73.1 ± 19.8 |
Table 6: Baseline characteristics of the two patient groups.
Furthermore, there was no significant deference in the history of cardiovascular risks between the ARB and Non-ARB groups as shown in the Table 7.
| Total | ARB Group | Non-ARB Group | |
|---|---|---|---|
| Type 2 Diabetes | 819 (66.7) | 411 (66.8) | 408 (66.6) |
| Renal factors - Elevated creatinine level - Protein urea - CKD stage 3 or more |
78 (6.4) 139 (11.3) 74 (6.0) |
43 (7.0) 64 (10.4) 40 (6.5) |
35 (5.7) 75 (12.2) 34 (5.5) |
| Cardiac factors - Myocardial infarction - Angina pectoris - Heart failure - Left ventricular hypertrophy - Transient or persistent atrial fibrillation |
54 (4.4) 114 (9.3) 43 (3.5) 172 (14.0) 87 (7.1) |
29 (4.7) 55 (8.9) 23 (3.7) 91 (14.8) 42 (6.8) |
25 (4.1) 59 (9.6) 20 (3.3) 81 (13.2) 45 (7.3) |
| Cerebral factors - Cerebral infarction - Cerebral hemorrhage - Subarachnoid hemorrhage - Transient ischemic attack |
98 (8.0) 13 (1.1) 8 (0.7) 48 (3.9) |
51 (8.3) 6 (1.0) 4 (0.7) 23 (3.7) |
47 (7.7) 7 (1.1) 4 (0.7) 25 (4.1) |
| Peripheral artery factors - lower extremities bypass surgery or angioplasty - Ankle-brachial index of <0.9 or with intermittent claudication |
3 (0.2) 4 (0.3) |
2 (0.3) 3 (0.5) |
1 (0.2) 1 (0.2) |
Table 7: Cardiovascular risks of the two patient groups.
To our knowledge, there is no report of the large-scale study that measures biomarkers in 1000 or more patients in the time course for 3 years like the ATTEMPT-CVD. There are many studied that elucidate the relationship between biomarkers and cardiovascular events. We are very interested in not only the levels of biomarkers at enrolment but also the changes of biomarker levels in patients suffering from cardiovascular events during the study period. We focus on the changes of plasma BNP and UACR levels in the present study because the efficacies that ARB improves those biomarker levels and the incidence of cardiovascular events are generally known. It is good opportunity for us to confirm whether the two markers sensitively change as predictive factors.
In the present study, we chose telmisartan as an ARB, because it was proven in the ONTARGET that termisartan had equivalent effects comparing to that of ACE inhibitor ramipril. Furthermore, of the components of the primary composite outcome, telmisartan reduced the incidence of myocardial infarctions compared to placebo group in the telmisartan randomised assessment study in ACE intolerant subjects with cardiovascular disease (TRANCEND) [27], although the power of ARB that reduces myocardial infarction is thought to be weak.
We selected urinary 8-OHdG, eGFR, serum adiponectin, high-molecular weight (HMW) adiponectin, serum hsCRP other than UACR BNP as biomarkers. 8-OHdG is an excellent marker of oxidative DNA damage, which increases in diabetes [28]. Recently, it was also shown that urinary 8-OHdG had a positive correlation with UACR in type 2 diabetics [29]. The association between 8-OHdG and UACR could be clear in the present study. Furthermore, eGFR is independently associated with heightened risk for death and hospitalization for heart failure in patients with chronic heart failure [30] and all-cause mortality in patients undergoing cardiac catheterization [31]. Adiponectin, the most abundant circulating adipokine, is paradoxically decreased in obesity, with the HMW adiponectin considered to be the biologically active moiety [32,33]. HMW adiponectin levels are associated with greater insulin sensitivity, antioxidative and anti-inflammatory effects [34,35], and consistently lower risk of future type 2 diabetes mellitus in prospective analyses [36,37]. In 2002, on the basis of data from 27,939 initially healthy women followed up over a decade, plasma levels of high sensitivity c-reactive protein (hsCRP) <1 mg/l, 1 to 3 mg/l, and >3 mg/l were established as representing lower, average, or higher relative vascular risk when added to traditional risk factors [38]. In an effort to improve vascular risk detection, many physicians screen for hsCRP, an inflammatory biomarker associated with a markedly increased risk of myocardial infarction, stroke, peripheral arterial disease, and sudden cardiac death [39]. These attractive and interesting markers are also investigated in the present study.
In conclusion, the ATTEMPT-CVD is a multicenter, prospective, randomized open-blinded end-point design study, and is the first study to assess the efficacy of ARB therapy to the changes of biomarkers in patients with high-risk hypertension through the time course, in terms of cardiovascular morbidity and mortality. Hence, the results of this study are expected to provide a novel insight into the significance of biomarkers considering the therapy on high-risk hypertensive patients.
This study is supported by the Japan Foundation for Aging and Health.
Dr Ogawa reported receiving grant support and lecture’s fees from AstraZeneca, Astellas, Bayer, Boehringer lngelheim, Chugai, Daiichi Sankyo, Dainippon Sumitomo Pharma, Eisai, Kowa, Kyowa Hakko Kirin, Mitsubishi Tanabe, MSD, Novartis, Otsuka, Pfizer, Sanofi, Sionogi, Takeda.
Dr Kim-Mitsuyama reported receiving grant support and lecture’s fees from Astellas, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Kyowa Hakko Kirin, Novartis, Sionogi, Takeda.
Dr Node reported receiving grant support and lecture’s fees from Astellas, Boehringer Ingelheim, Daiichi Sankyo, Kowa, Merck, Mitsubishi Tanabe, Novartis, Pfizer, Takeda
Dr Yasuda reported receiving grant support from Bayer, Boehringer Ingelheim, Mitsubishi Tanabe, Shionogi.
No other conflicts were reported.