Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2013) Volume 0, Issue 0
One of the characteristics that defines many malignancies that metastasize via the circulatory system, is their ability to shed surface membrane proteins into the blood stream where they can be detected as tumor markers. The primary clinical application associated with defining these tumor markers, many representing carbohydrate antigens, has been in their use for specifically monitoring the status of the patient, in terms of their response to therapy. In the more than 40 years of the clinical measuring what we term tumor markers, none have been defined that are of value in their ability to help the clinician to diagnose the presence of an existing malignancy. Rather, their role has been assigned to that of a monitoring function. It appears essential that the ideal tumor marker, when defined, should be able detect the presence of an established tumor, as well as characterize the clinical state of such an existing neoplasm. This same marker should more importantly be expressed only in the malignant state and not be associated with inflammatory conditions developing in normal tissue adjacent to the tumor. In general, those markers presently available for clinical use are carbohydrate in origin, showing up in many conditions unrelated to the presence of cancer. Their use has been relegated to monitoring the clinical course of a known malignancy in terms of response or lack of to a therapeutic approach: that is radiation or chemotherapy. When the proper target proteins which are in the process of being defined and are detected by monoclonal antibodies directed against a specific epitope on the protein, the same monoclonal used for detection, when delivered intravenously can hunt, seek and destroy the existing neoplasm.
<Keywords: Tumor markers, Monoclonal, Epitope, Chemotherapy
In following the clinical course of a patient with pancreatic cancer, the approach we employ today, subsequent to having obtained a biopsy for tissue diagnosis, is to use of an array of monoclonal antibodies for detecting the presence of potential circulating tumor markers. The more common antibodies (mAb’s) used in defining such markers are CA.19.9 as well as CA-50, CA-195, and TATI [1]. Many of these above noted markers have cross reactivity with other tumors as well as inflammatory situations arising in normal tissue minimizing their true value.
Our group has been interested in defining better targets that are more specific to defining the presence of pancreas cancer without showing cross reactivity to targets found in normal or inflammatory pancreatic tissue. We have been able isolate, define and characterize several such tumor membrane proteins that proved to be immunogenic and showed no evidence of cross reactivity to normal tissues.
The process of searching for and defining the presence of serum protein targets that characterize the status of a malignancy was initiated with the recognition of the tumor protein CEA, a marker that could be detected in the serum of patients with various forms of malignancy [2]. Later, a number of additional serum tumor markers were recognized that shed into the serum under an array of different clinical situations. Most represented carbohydrate molecules. In the intervening years these shed cancer (markers) molecules defined by their corresponding antibodies, were found to represent for the most part, molecules derived from the surface membrane of colon cancer cells (CA 17.1A), pancreas cancer (CA 19.9) and ovarian cancer, (CA125) as these tumor invaded the blood stream.
The prefix CA has been, for the most part, misinterpreted by many to represent the term Cancer Antigen when in effect it pertains to Carbohydrate Antigen as the type of marker, one that is seen expressed in both the malignant as well as the inflammatory state of the tissue. The tests that were developed for defining these serum carbohydrate markers eventually became commercially available in spite of their lack of specificity for the malignant state of disease. As an example, it has recently been shown that the use of PSA monoclonals like those of the other CA antibodies have a high degree of inaccuracy in terms of cancer diagnosis. As such most carbohydrate tumor markers have been relegated specifically to monitoring the clinical status in terms of the response to various therapeutic applications. Here, a rising marker associated with a history of a previous malignancy suggests progression of disease whereas lowering of the CA marker suggests a potential response, most likely due to the use of radiation or chemotherapy.
In no instance, where a specific circulating marker was detected, could the corresponding CA antibody that was used for monitoring, be employed as a therapeutic agent with the intent of targeting the marker to induce apoptosis in the associated malignancy. This would be the ideal use of a diagnostic monoclonal, one that could detect a tumor marker in-vitro serum ELISA and if necessary when given intravenously, hunt to destroy the cell expressing the tumor marker.
In pancreatic cancer, as the molecular process associated with the transformation to malignancy evolves, we have found that those intraepithelial cells involved in the process of transformation begin to express Tumor Associated Antigens (TAA’s). These TAA proteins have been found to be relatively specific to the neoplasm, not being seen in adjacent normal tissue. We have been able to determine that the proteins that we have identified and that appear specifically in pancreatic cancer as well as in other G.I. malignancies, serve both as markers to identify the malignancy by serum ELISA as well as by Immunohistochemistry (IHC). The latter procedure has been useful in illustrating that when the tumor marker is expressed in the tumor cellular structure; there is no evidence of its appearance in the adjacent normal tissue. These tumor markers have also helped by serving as immunologic targets for tumor destruction [3].
The tumor proteins that we have become interested in have been shown for the most part to be oncofetal in origin. They appear early in the genotypic transformation of the normal pancreatic acinar cells as it takes on the characteristics of the malignant state. These same proteins can then be shown to serve as specific tumor markers that shed into the serum as invasion of circulatory and lymphatic system takes place.
The immunogenic tumor proteins that we have identified and are being employed by our group in studying in pancreatic cancer; serve both as tumor markers by ELISA and IHC. They were first identified by Hollinshead et al. [4] from pooled allogeneic tumor specimens obtained following surgery. Further purification by sephadex column chromatography and isoelectric focusing led to the identification of these tumor associated antigens. Patients were then skin tested for specificity of these antigens evaluating their delayed (cutaneous) hypersensitivity responses, DHR, in an array of different malignancies as well as in normal patients, to assure that those proteins being defined, represented the specific immunogenic Tumor Associated Antigens (TAA). In order to further define and to sequence these proteins, monoclonal antibodies were developed. They allowed for immunopurification and mass spectroscopy [5]. The resulting sequences of the tumor antigens characterized as NPC- 1, NPC-2 (31.1) and 16C3 were eventually shown to represent the mutated or post translational modified oncofetal forms of MUC5ac, A33 and CEA cam [5]. Modifications in structure of these antigens were usually found to occur in the core peptide sequence.
We then utilized Immunohistochemistry (IHC) to define antigen distribution in the pancreatic tumor specimens being studied. In each tumor being evaluated, either one or a combination of two monoclonals, showed the presence of these tumor associated antigens. In over 100 tissue samples examined in our lab, the Immunoperoxidase activity per mAb utilized, yielded positive staining results ranging from 64% to over 97% of the cases evaluated [5]. When used in combination, virtually all tumor specimens were positive by IHC. Essentially, no cross reactivity to normal tissue were seen. The exception appeared to occur when genotypic transformation appeared in the normal cells adjacent to the tumor. This was noted when several pancreatectomy patients had evidence of local recurrence where the transected neck of the pancreas was implanted into the jejunum. Immunostaining showed that what appeared to be normal pancreatic cells adjacent to the primary lesion did express the same antigen as the primary malignant lesion did. Similarly we went on to utilize the ELISA procedure to Monitor the shedding of those tumor antigens that we had defined, into the serum.
Measurement of our three Tumor Associated Tumor Antigens (TAA) markers shed from tumor into the serum from pancreatic cancer, have been performed using an ELISA protocol. The Indirect ELISA is commonly employed in our lab along with the sandwich ELISA which is now standardized in the Precision laboratories. Levels below 100 μg/ml of serum antigen are considered normal where most patients with active pancreatic malignancy have levels approximating 1000 μg/ml or higher.
The ELISA, An enzyme linked immune absorbent assay, uses one type of heterogeneous, solid phase enzyme immunoassay (EIA) to detect the presence of a substance (usually tumor antigen shed from the metastatic lesion) in a liquid sample such as serum. In this more common study, an unknown amount of antigen is affixed to a surface and then a specific antibody is applied to that surface to allow it to bind to the antigen. The antibody employed is linked to an enzyme and following this application, a substance containing the enzyme substrate is added. The ensuing reaction produces a color change that can be measured as a reflection of the quantity of antigen that was detected.
We presently employ the “Sandwich ELISA”, where the surfaces of the plates are coated with a known quantity of capture antibody. Antigen containing sample such as an unknown serum sample is applied to the plate. The latter is then washed to remove unbound antigen. A specific antibody is then added and binds to the antigen which is stuck between the two antibodies. An enzyme liked secondary antibody is added that also bind specifically to the antibodies’ Fc region. A secondary chemical is then added that is converted by the enzyme into a color for quantitative measurement. When we first began employing the serum ELISA for diagnosis, testing a variety of serum samples of patients with colorectal as well as pancreatic cancer, initial results were extremely accurate, probably reaching to the level of high 90%+ specificity and sensitivity. It then became apparent that we were finding some false negatives that proved to be related to the nature of the monoclonal we employed. These mAbs were in the humanized format, taken from the batches used for therapeutic trials. In some patients, a rheumatoid or similar factor was present which bound to the human Fc of the Precision mAbs resulting in interference with the proper response to the reaction. As such we have reengineered the mabs employed in the ELISA so that a murine version is now being expressed in a separate clone of CHO cells transfected with the human Fab along with the mouse Fc. For immunohistochemistry, it is possible to continue using a chimeric version. In all preparations used in a kit form for staining, positive and negative controls must be employed.
As a result of early studies by our scientific group, the pancreatic tumor markers we have isolated and characterized were found to serve a dual role as mentioned previously, first by defining a diagnostic marker present in tumor which then shed into the serum and then secondarily by serving to attack the marker expressed in the tumor as a therapeutic target. Hartwell [6] appeared to support the need for specifying diagnostic antibody activity early in the transformation process wherein an early tumor marker could be demonstrated by IHC at a time when phenotypic appearance of the cell appeared normal. Figure 1 summarizes the Hartwell approach to diagnose with the potential for possible therapy to follow as described by Norton in the same meeting.
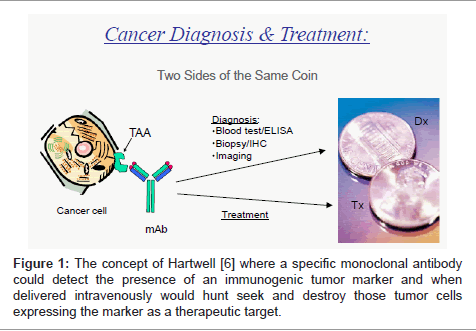
Figure 1: The concept of Hartwell [6] where a specific monoclonal antibody could detect the presence of an immunogenic tumor marker and when delivered intravenously would hunt seek and destroy those tumor cells expressing the marker as a therapeutic target.
The characteristics of a true tumor marker have to be carefully considered since the search for newer and more specific ones continue at many cancer research facilities. The criteria here should be that the marker be a protein or glycoprotein that is expressed in the malignancy only, can be identified when invasion of the circulatory system has occurred via a serum ELISA, both for diagnosis and monitoring, and that the antibody to the marker has the ability to induce ADCC (antibody dependent cell cytotoxicity) when delivered intravenously (Table 1). Tumor destruction should then be seen in those cells expressing only target antigen. The rationale for failure of the immune system to control tumor growth in a host harboring a malignancy is probably related to the fact that the host has not encountered sufficient levels of immunogenic tumor protein shed from the malignancy to turn on an adequate antitumor response. Rather, the immune system for the most part only detects the presence of a relatively small level of tumor antigen, and exerts a minimal response through a process termed “tumor surveillance”. In the original Hollinshead et al. [4] vaccine trials, it was shown that an ideal response to tumor antigen occurred with the administration of a threshold level of approximately 750-1000 μg of antigen administered intradermally along with an adjuvant. In most malignancies the level of immunogen (TAA) expression rarely exceeds 30-50 μg. An evaluation of the mechanism by which the TAA vaccine induced an immune response enhancing survival of the patient being treated proved to be that of an enhancement in antibody production with minimal participation of the cytotoxic T cells. This led to our investigation of the mechanism of antibody response to the presence of the tumor and its ability to detect the antigen both as expressed by the tumor and the result of its presence in the serum [7].
| E/T | ASPC-1 | CF-PAC-1 | SW-1463 | SK-Mel |
| 100:1 | 41.1 | 32.5 | 23.6 | -0.8 |
| 50:1 | 26.1 | 17.5 | 15.2 | -0.2 |
| 25:1 | 17.4 | 8.2 | 6.8 | -0.4 |
| 12.5:1 | 9.0 | 4.8 | 1.5 | -2.1 |
Table 1: Illustrating ADCC using one of the specific pancreatic monoclonal
antibodies NPC-1.
Of secondary but of clinical importance, is the time at which a marker is first expressed in the tumor. We have found, after studying a large array of neoplastic lesions that the ideal tumor marker appears at the time of the initial genotypic transformation, when in many cases the marker can be detected 4-6 months prior to the histologic identification of the presence of the malignant process. As such, when examining normal margins of resection following a Whipple pancreatectomy by immunohistochemistry, those margins examined by frozen section frequently demonstrate the presence of tumor antigen expressed in benign appearing cells. Such cells, as previously mentioned, are the probable cause of anastomotic or suture line recurrence for both colon and pancreas cancers.
Origin of the diagnostic/therapeutic tumor markers expressed in pancreas cancer
Those pancreatic tumor glycoproteins representing immunogenic molecules expressed in pancreatic cancer are present as oncofetal proteins expressed in the developmental stage of the fetus, and appear important as the GI tract matures. One such glycoprotein in particular, MUC5AC, which is expressed early in fetal life, is associated with the expression of mucin in the tracheobronchial tree as well as colon and pancreas, helping in the needed function of those organs as the fetus matures. At birth, the gene expressing the needed mucinous product is remethylated to prevent past pointing the fetal needs of such gene products. As such, when mucin levels continue to be expressed in the newborn and exceed the physiologic need, failure to have remethylated the MUC5AC gene results in the clinical appearance of cystic fibrosis. Later in normal pancreatic tissue, if viral transfection or a carcinogenic effect takes place, a mutated or post translational modification in the core peptide of MUC5ac results, rendering the molecule an immunogenic tumor associated antigen. The two other proteins as noted before are variants of A33 fused to an exosome and 16C3 related to the CEA class of CEAcam 5 and 6 [8]. Here these variants of tumor antigen are exceedingly immunogenic and serve as excellent markers for defining pancreatic cancer. As the tumor grows from its intraepithelial state over a 15-20 year period of time, it eventually invades the basement membrane of the pancreatic duct, becomes highly aggressive and tends to metastasize readily. At this point the shed membrane tumor markers appear in the blood stream where they can be identified by ELISA. Use of CA antibodies as the present day standard however, have a high level of inaccuracy in diagnosing a lesion as one that is malignant vs. an inflammatory process since they are measuring levels of carbohydrate antigen. By utilizing the pancreatic tumor protein markers that we have described, as a target of identification, we have been able to define and diagnose the presence of pancreatic carcinoma with better than 90% specificity and sensitivity.
Standards for improving the role played by tumor markers have appeared and basically state that a tumor marker as employed in the diagnosis and monitoring of malignancies should be defined as a naturally occurring molecule that is measured in the serum, plasma, or other body fluids as well as in paraffin embedded tissue to identify the presence of cancer, to assess patient prognosis or to monitor a patients response to therapy with the overall goal of improving the clinical management of the patient [9,10].
The first tumor marker to be utilized for the possible detection of cancer was CEA, a protein isolated, characterized and developed by Phil Gold. It has been used in serum ELISAs for many years, but like the carbohydrate antibodies, it was found to have its primary value in monitoring the response or lack of response to a defined form of treatment affecting the malignancy. Because of its presence in normal bowel and other organs, certain activities such as smoking or use of an enema can be associated with an elevated serum level. A variant of the CEA molecule, a mutated form of CEAcam 5 and 6 has been shown to have both diagnostic and therapeutic value [11].
The CA 19.9 tumor marker and its associated monoclonal , frequently used as a marker for pancreatic cancer , has become the standard for following pancreatic neoplasms, but again is best utilized for immune monitoring. Too many unreliable interpretations have been made when the marker is identified in the diagnostic setting.
Other pancreatic markers such as Serum APRIL, represent another entry into the list of markers to be evaluated. It has been considered to be one of the newer potential tumor markers for pancreatic cancer. This marker, representing A Proliferation Inducing Ligand (APRIL) is a member of the Tumor Necrosis Factor (TNF) super family. It essentially is over expressed [12] in pancreatic cancer but only weakly if not at all in the normal pancreatic glandular tissue. The marker was found to be increased in patients with pancreatic cancer which proved to show positive correlation with CEA and CA19.9 levels in the serum The sensitivity of April alone in diagnosing the presence of malignancy was 70.1% when compared with that of CEA alone (56.7%) and similarly somewhat better than CA 19.9 alone. The sensitivity increased when APRIL was used in combination with CA19.9 reaching a level of 88.1% [12].
In another study analyzing various serum protein changes that could be defined during the development of pancreatic cancer, an alteration in haptoglobin structure and levels thereof were seen. Such variations occurred in the sugar groups that were attached to the haptoglobin. These variations were identified by mass spectroscopy. It was found that it was easy to identify changes in the structure of the sugar groups. These changes were either structural or quantitative and found to be present for each stage of pancreatic cancer vs. pancreatitis, diabetes or from normal serum samples [13]. When evaluated in a group of 149 patients prospectively, acute phase reactants such as haptoglobin and Serum Amyloid A (SAA) were significantly elevated in those patients with pancreatic adenocarcinoma when compared to those with chronic pancreatitis as well as healthy controls. Haptoglobin was superior to SAA when differentiating pancreatic cancer from other benign conditions of the pancreas. The sensitivity and specificity of haptoglobin was found to be 82.7% and 71.1% respectively. Although these results remain inferior to CA 19.9 as a standalone marker, when used in combination, the sensitivity of 81.3% and specificity of 95.5% is a measurable improvement [14]. We have stated on numerous occasions that one of the important characteristics of a functional monoclonal antibody used to target a serum marker specific to a malignant lesion, is its ability to identify the marker within the tumor by IHC and to then demonstrate that the marker is shed from the surface of the tumor into the serum. Carbohydrates are frequently shed from the tumor surface into the serum, but when the equivalent monoclonal is used for defining its existence in the tumor, one sees cross reaction to an array of normal tissues where their inflammatory components similarly shed the carbohydrate maker found on their surface, into the serum. The specificity of Precision mAbs targeting pancreatic cancer and not to normal cells is seen in the illustration in figure 2.
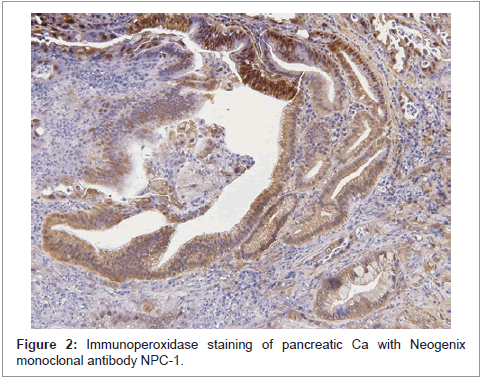
Figure 2: Immunoperoxidase staining of pancreatic Ca with Neogenix monoclonal antibody NPC-1.
The above illustration clearly identifies tumor cells expressing tumor associated antigen (TAA) before invasion into surrounding parenchyma has occurred. In this case the tumor antigen that was targeted, proved to be the oncofetal protein associated with the mutated/altered form of MUC5ac. False positives have not been seen in the numerous sections studied to date when our monoclonals are utilized. In certain instances when examining cells at the margins of the malignant growth, transitional cells can be found that have been modified genotypically, but still have a normal phenotypic appearance. At times, during microscopic examination antigen has been seen to shed from the glandular component of the tumor, shedding into the lumen and eventually accumulating in the ductal system of the pancreas. As the tumor becomes more aggressive and invades stroma to actually compress the microcirculation, minimizing blood flow, delivery of chemotherapy is impaired but can be assisted if certain agents modifying the stroma and increasing blood flow is utilized. The classic appearance of a more advanced lesion stained by IHC is seen in figure 3.
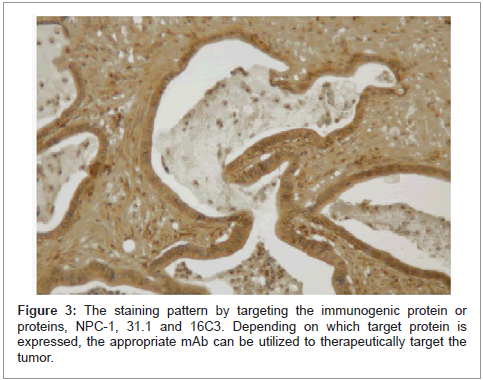
Figure 3: The staining pattern by targeting the immunogenic protein or proteins, NPC-1, 31.1 and 16C3. Depending on which target protein is expressed, the appropriate mAb can be utilized to therapeutically target the tumor.
In evaluating the NPC-1 antibody targeting MUC5ac for an FDA therapeutic IND in metastatic pancreatic cancer, multiple normal tissues required for the study failed to react with NPC-1 essentially indicating the specificity of this as well as our other mAbs for targeting the tumor only. When normal pancreatic tissue adjacent tumor is found to express antigen, it is for the most part due to the presence of tumor protein in those cells undergoing transformation into the malignant phenotype. As such, at the time of a Whipple resection, it is of value to examine the transected margin of the head/neck region by immunohistochemistry.
A number of additional as well as potential serum markers for pancreatic cancer have included Pancreatic Oncofetal Antigen (POA), DU-PAN, and osteopontin [15]. The marker antibodies to date continue to recognize carbohydrate rather than protein epitopes and as such elevations are frequently seen but related not to the presence of a malignant lesion but to inflammatory conditions of a non malignant nature occurring in the pancreas and other tissues.
A combination of SDS-PAGE and blotting with a panel of lectins chosen to identify different carbohydrate epitopes, have demonstrated the presence of a high MW glycoprotein in approximately one-third of pancreatic cancer serum but in no control sera. The marker proved to be a mucin which was developed into an Enzyme Linked Peanut Lectin Assay (PNA-ELLA) for total peanut lectin binding glycoprotein measurement in serum [16]. In combination with CA 19.9, the two have a combined sensitivity of 85% in pancreatic cancer serum [17]. Ca 19.9, as with many of the Precision Biologics anti-colon/pancreatic cancer markers was originally raised against colorectal cancer. In contrast to the Precision antibodies targeting tumor shed Antigen, Peanut Actin (PNA) binding glycoprotein is present in normal pancreatic tissue, inflammatory tissue as well as carcinoma. Both serum and tissue PNA binding glycoproteins have identical electrophoretic mobility.
There has been some interest in the evaluation of CA 242 as a marker for pancreatic cancer. However the specificity was significantly lower (80%) than that of CEA and CA 242, 92% when the latter two markers were used in combination. Furthermore those with high CA 242 levels had a remarkable shorter survival time. However in the study reported by Ventrucci et al. [18] in Clinical Chemistry and Lab Medicine 2012, the serum CA 242 was further investigated in the hopes of effectively searching for a valid marker of pancreatic cancer. The sensitivities reported for CA 242, CA19.9 and CA 50 were 41.3%, 54.3% and 47.8 % respectively in an array of 276 subjects with various combinations of inflammation, cancer and healthy subjects. No significant improvement was achieved by using combinations of the CA 242 with CA19.9, Ca 19.9. the sialylated Lewis blood group antigen, remains one of the primary current markers employed in following the clinical course of pancreatic adenocarcinoma. Results were found to be suggestive of malignancy when the patients for the most part, had symptoms of the disease. In a study of 261 such patients the sensitivity was 70% and specificity 87%. For small tumors less than 3 cm, the sensitivity decreases to about 55%. A mean serum concentration in asymptomatic individuals was 9.4 U ± 9.9 U/ml., where finding levels of at least 37 U/ml and greater were more accurate when discriminating pancreatic cancer from benign pancreatic disease. In situations where biliary obstruction, chronic pancreatitis and acute cholangitis were present, high titers of the marker were noted, suggesting that the CA 19.9 marker best fit in monitoring rather than in diagnostic situations. This holds true for most if not all CA markers as typified by the carbohydrate marker PSA for defining prostate cancer which is now falling into disrepute as a valid diagnostic marker. At Johns Hopkins, a number of markers have been explored for evaluating the presence of pancreatic cancer. In 2004, they reported the possible use of mesothelin, as a serum marker to define pancreatic cancer [19]. The marker also appeared in the serum of patients with ovarian and lung cancer. While the antigen is somewhat immunogenic, no correlation with use of the mesothelin monoclonal antibody and tumor response has been reported. When MUC-1 was studied as a serum marker the presence of the target antigen was able to distinguish not only cancer from normal, but cancer from chronic pancreatitis. Combinations using CEACAM1 with CA19.9 were first reported to be superior to using each individually but when further evaluation was carried out; this combination was no better that CA 19.9 when used alone.
Brand et al. [20] performed an immunoassay utilizing 83 different markers including amylin, CA 19.9, ICAM-1.OPG, and TIMP. He included 333 patients with pancreatic cancer, 144 patients with benign pancreatic disease and 227 healthy controls. When they compared a combination panel including, as most studies do, CA 19.9 along with ICAM-1 and OPG, they reached a sensitivity and specificity of 78% and 94% respectively at detecting the pancreatic cancer lesion. They also noted that these results were superior to using the CA19.9 alone. [21] Other attempts at using known protein mutations occurring in pancreatic Ca have been tried such as the evaluation of KRAS and its associated mutations [22]. A ligAmp assay of the KRAS sequences appearing in bile was performed by Shi et al. suggesting a relatively good level of specificity and sensitivity approaching 90% [23]. The ability to detect mutant KRAS however is currently not popular since less than 50% of existing mutations are detectable by the established assays.
More complex approaches have been employed in the hopes of defining more specific markers indicating the presence of pancreatic cancer. Protein profiling using Surface-Enhanced Laser Desorption Ionization Time of Flight Mass Spectroscopy (SELDI_TOF-MS) and Protein Chip analysis was 18 employed in evaluating samples from twenty patients who under surgical resection of pancreatic neoplasms. Sequential amino acid analysis revealed the protein of interest to be Apolipoprotein C-1 [24]. This marker appeared to indicate some usefulness as a prognostic marker of pancreatic cancer where CA 19.9 showed no correlation with the disease free and overall survival time in the twenty patient studies.
Insulin like Growth Factors (i.e. IGF-1) and their binding proteins, IGFBP 1 and 3, have been found to play a significant role in regulating cell differentiation, proliferation, and apoptosis. The circulating levels of these markers have been implicated in several studies as an accurate diagnostic tool for pancreatic cancer. In a prospective case controlled trial of 144 patients matched with 429 controls, investigators showed that only subjects in the lowest quartile of plasma IGFPB-1, experienced an elevated risk of pancreatic cancer. These findings were confirmed in several other prospective cohort studies [25].
In another study out of Johns Hopkins [26] in 2006 investigators analyzed five new candidate serum mariers in hopes of finding a useful standalone and an early predictor of pancreatic cancer. Fifty patients with pancreatic cancer were matched with controls having known pancreatitis. CA 19.9, MIC-1 (macrophage inhibitory cytokine-1), osteopontin, tissue inhibitor of metalloproteinase 1, and hepatocarcinoma-intestine-pancreas protein levels were all evaluated for their potential significant value as genuine markers. MIC-1 and CA 19.9 were the only ones when employed as markers that significantly predicted a probable diagnosis of pancreatic carcinoma. Although MIC-1 better differentiated patients with pancreatic cancer from healthy controls, it did not adequately distinguish chronic pancreatitis from pancreatic cancer considering that one of the antigens of importance being defined by the Precision Biologics monoclonals is a MUC protein, it was interesting to note that Wang described the presence of MUC4 as a potential pancreatic marker [27]. However, while this protein is aberrantly expressed in pancreatic adenocarcinoma and undetectable in normal and inflammatory pancreatic tissue, its measurement by RAI and ELISA has proven to be unsuccessful. In its place, a Surface Enhanced Raman Scattering (SERS) based immunoassay was used to detect MUC4 with more success and when serum from the cancer patient was compared to normal serum, the MUC4 antigen marker appeared to be significant as a potential marker for identifying pancreatic carcinoma in some state of active disease.
Obviously, in looking at the mutated or modified form of MUC5ac along with the other TAA glycoproteins that we have defined in pancreatic cancer, it is apparent that these glycoproteins meet Hartwells definition of an effective tumor marker that appears to be expressed early in the transformation of the normal cell to malignancy, and serves as a good marker by IHC as well as for use in serum testing. From our point of view these markers also serves as potential targets for eventual tumor destruction by immunotherapy using the chimeric/ humanized version of diagnostic monoclonal antibodies that we have developed. When the tissue of interest is examined and blood samples are analyzed by ELISA so that the proper target antigen is determined to be present, these diagnostic monoclonals can change their role to that of therapeutic agents. This therefore ties into the nature of the immunogenic tumor markers being targeted and how they respond in the overall picture of Theranostics. We anticipate that the methods we are developing and employing in the clinical situation will become a part of the overall approach toward controlling pancreatic and other malignant disease processes.