Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2014) Volume 3, Issue 3
Background: The diffuse sclerosing variant of papillary thyroid carcinoma (DSV) is a rare subtype of papillary thyroid carcinoma (PTC), and the prognosis of patients with this variant is not yet fully understood. The aim of this study was to determine whether DSV is a poorer prognostic factor than non-DSV.
Methods: We reviewed the histologic slides of 12,664 primary PTC cases and divided them into DSV and non- DSV groups. Based on the results of the follow-up study and the age distribution of patients, we selected the data from 810 female patients and compared outcomes between patients with DSV and patients with non-DSV.
Results: Of all initial patients, 43 had DSV. Of these, 4 patients were deceased, and 39 were alive with a mean survival of 11.1 ± 9.7 years (mean ± SD) after surgery; the deceased patients were all female patients with papillary non-microcarcinoma (PNMC, >10 mm diameter). A substudy of female PNMC patients by age showed that a cutoff at age 33 years was optimal for analyzing the DSV and non-DSV groups. Of 810 female patients younger than 33 years with PNMC, 25 had DSV and 785 had non-DSV. Of the patients with non-DSV, 23 patients died, including 5 deaths from PTC. The overall mortality and disease-specific mortality rates of the selected patients were not statistically significant between the DSV and non-DSV groups (2/25 vs. 23/785, p=0.18 and 1/24 vs. 5/767, p=0.17, respectively).
Conclusion: DSV is not an aggressive subtype of PTC and patients with DSV do not require more aggressive therapy than patients with non-DSV of the same stage.
In 1953, Crile and Fisher were the first to report papillary thyroid carcinoma (PTC) diffusely intermingled with chronic thyroiditis [1], which was later named diffuse sclerosing variant of papillary thyroid carcinoma (DSV) [2]. In 1989, Carcangiu and Bianchi characterized the various histological findings of DSV, which include diffuse involvement of one or both lobes, numerous micropapillary formations located within cleft-like spaces consistent with lymph vessels, extensive squamous metaplasia, large number of psammoma bodies, marked lymphocytic infiltration, and prominent fibrosis; of these, intrathyroidal lymphatic permeation was thought to be the most important feature of DSV [3].
The clinicopathologic characteristics of DSV are now well established [4], but the prognosis of patients with DSV remains uncertain [4,5]. For this reason, this study was undertaken to determine whether DSV is a poor prognostic subtype of PTC.
Between January 1971 and December 2013, 12,662 consecutive patients with primary PTC underwent initial surgery at Noguchi Thyroid Clinic and Hospital foundation. Except for patients with incidental PTC (PTC first found at the postoperative pathological examination), they were treated with conventional treatment for PTC, and postoperative radioiodine ablation therapy was not performed. Subtotal thyroidectomy with a modified radical neck dissection is our standard procedure for papillary thyroid carcinoma [6].
We reviewed the histologic specimens of these patients and divided the cases into DSV and non-DSV groups according to the 2004 World Health Organization Classification of the Tumors [4]. Papillary thyroid carcinoma with lymphatic permeation was diagnosed as DSV (Figure 1). The sex ratio, age distribution, and ratio of patients with papillary microcarcinoma (PMC, ≤ 10 mm diameter) to patients with papillary non-microcarcinoma (PNMC) were compared between the 2 groups.
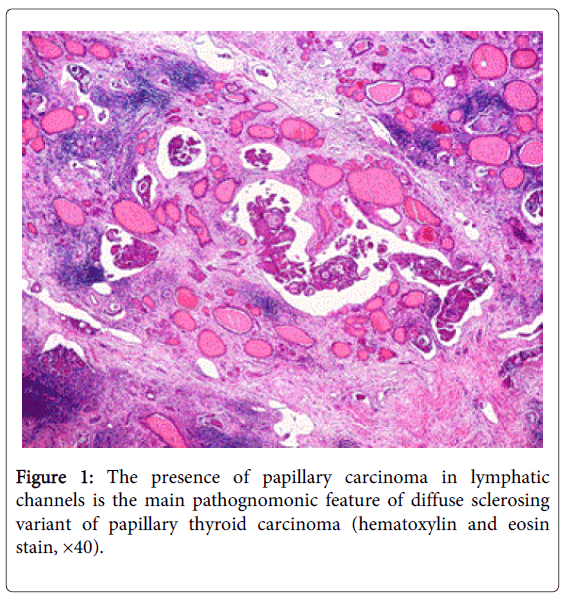
Figure 1: The presence of papillary carcinoma in lymphatic channels is the main pathognomonic feature of diffuse sclerosing variant of papillary thyroid carcinoma (hematoxylin and eosin stain, ×40).
Age was determined by each patient’s age at the time of the first surgery. Tumor size was determined by the largest diameter of the tumor measured on the macroscopic cut surface. When 2 or more cancer nodules were detected in one case, the size of the largest nodule was used. Cases of DSV involving an entire lobe(s) were classified as PNMC.
Follow-up study typically occurred as follows. During the first 2 years after discharge, patients were examined for recurrence and distant metastasis twice a year at the outpatient clinic, and if no events occurred during this period, they were evaluated once a year. When patients came not to visit the out-patient clinic, we performed a questionnaire survey once a year. Dates and causes of death were obtained from the death certificate and the Japanese family registry, and information about the final hospital stay was obtained from the patients’ doctors and families. The follow-up rate for patients with thyroid malignancy was more than 95%.
Based on the results of the follow-up study and the age distribution of patients, we focused our study on female patients younger than 33 years with PNMC. We compared disease free survival periods, the overall mortality, and disease-specific mortality rates of these patients with DSV to these patients with non-DSV.
We used a statistical software program (JMP 8.0; SAS Institute Inc., Cary, NC, USA) for data analysis. All statistical tests were two-tailed.
Of the initial group of 12,662 patients with PTC, 43 patients, including 3 male patients, had DSV. The incidence of DSV among patients with PTC was 0.3% (43/12,662), and excluding patients with PMC, the incidence was 0.6% (38/6,603).
Of the 43 patients with DSV, macroscopic figures of the cut surface were available for 25 cases. No dominant nodule, a dominant nodule with a blurred margin due to tumor cell invasion, and a dominant nodule with a clear margin were found in 3, 8, and 14 cases, respectively
Table 1 summarizes the age distribution, the female to male ratio, and the PMC to PNMC ratio of patients with DSV and patients with non-DSV. Patients with DSV were much younger than those with non-DSV. Female patients were predominant in both groups, and the difference in sex ratio was not statistically significant. The ratio of PMC to PNMC was lower in the DSV group.
| DSV | Non-DSV | P | |
|---|---|---|---|
| Age (y, mean SD) | 33 15 | 5114 | <0.001 |
| Female/male ratio | 40/3 | 10972/1647 | 0.3604 |
| PMC/PNMC* ratio | 5/38 | 6054/6565 | <0.001 |
*PMC, papillary microcarcinoma; PNMC, papillary non-microcarcinoma; DSV, diffuse sclerosing variant of papillary thyroid carcinoma
Table 1: Comparison of patients with DSV and non-DSV
All 43 DSV patients had follow-up. The mean follow-up period was 11.7 ± 10.5 years (mean±SD). During this period, 8 patients had nodal recurrence, 1 patient had distant metastasis (pulmonary), and 4 patients died. All deceased patients were women with PNMC.
Table 2 shows the age at the initial surgery, the duration of survival after surgery, and the causes of death of these 4 patients. Two patients died within 5 years of the initial surgery, and other 2 died more than 30 years after the initial surgery. The cause of death was related to thyroid carcinoma in 1 patient, not related to thyroid carcinoma in 2 patients, and difficult to determine in 1 patient (the third patient in Table 2). The first patient in Table 2 had advanced cancer (stage 4) at the initial presentation. She underwent palliative surgery with tracheostomy and died 2 months after surgery owing to invasive growth of PTC. The second and fourth patients showed neither nodal recurrence nor distant metastasis and died of other causes. The third patient developed regional nodal recurrence 8 years after surgery and pulmonary metastasis 12 years after surgery. This patient’s nodal recurrence was successfully surgically removed, and the pulmonary metastasis was treated several times with radioiodine. The metastatic pulmonary nodules diminished in size but did not disappear completely and remained without re-growth. This patient’s serum thyroglobulin (TG) levels were high, with a final serum TG level of 5100 mg/ml at the age of 32. She died at the age of 46. According to a physician at a referring hospital, her cause of death was multiple organ failure initiated by interstitial pneumonitis and was probably not related to pulmonary metastasis of PTC. For our analysis, however, we made the assumption that she had died of DSV.
| Age at surgery (y) | Survival duration (y) | Cause of death |
|---|---|---|
| 66 | 0.2 | DSV |
| 31 | 4.8 | Accident |
| 16 | 31.0 | Multiple organ failure |
| 44 | 33.2 | Dilated cardiomyopathy |
Table 2: Fatalities among patients with DSV, listed in order of survival.
As shown in Table 1, patients with DSV were much younger than patients with non-DSV, and age is a major prognostic factor of PTC. For this reason, a substudy of female patients with PNMC was performed according to patient age. As shown in Figure 2, an age cutoff of 33 years was optimal for analyzing the DSV and non-DSV groups.
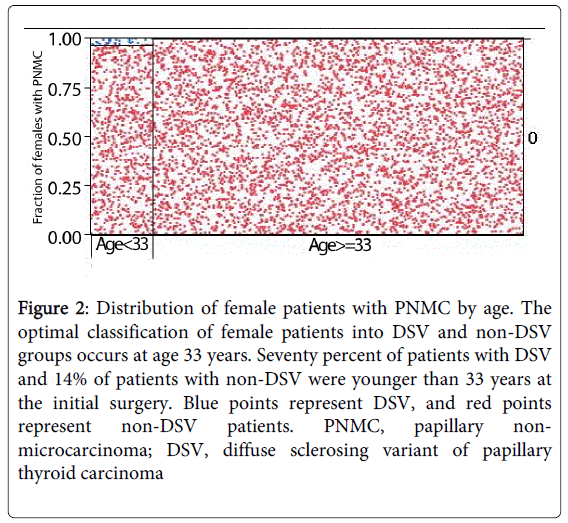
Figure 2: Distribution of female patients with PNMC by age. The optimal classification of female patients into DSV and non-DSV groups occurs at age 33 years. Seventy percent of patients with DSV and 14% of patients with non-DSV were younger than 33 years at the initial surgery. Blue points represent DSV, and red points represent non-DSV patients. PNMC, papillary nonmicrocarcinoma; DSV, diffuse sclerosing variant of papillary thyroid carcinoma
A total of 810 female patients under the age of 33 with PNMC were selected for the substudy analysis. Of these patients, 25 had DSV and 785 had non-DSV.
Figure 3 shows the disease-free survical curves of the 810 patients. Disease-free survival rate of DSV was significantly worse than that of non-DSV by Wilcoxn test (P value, 0.001) but not singnicantly worse by log-rank test (P value,0.17).
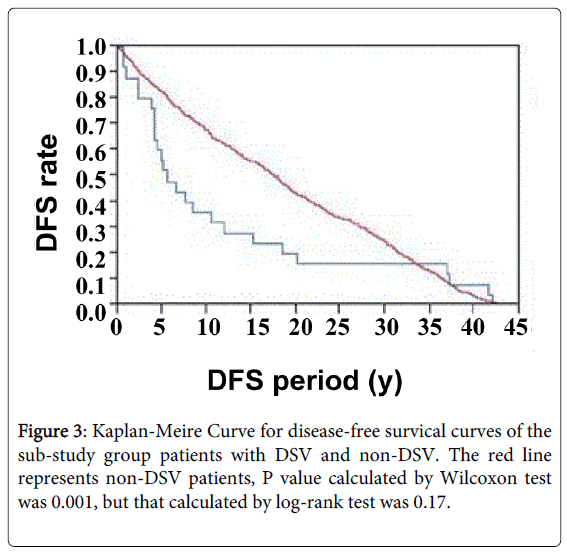
Figure 3: Kaplan-Meire Curve for disease-free survical curves of the sub-study group patients with DSV and non-DSV. The red line represents non-DSV patients, P value calculated by Wilcoxon test was 0.001, but that calculated by log-rank test was 0.17.
Of those with non-DSV, 23 died, including 5 deaths from thyroid carcinoma. Their ages were 15, 27, 29, 32, and 32 years at the time of initial surgery.
The overall mortality rate of patients selected for the substudy was 2/25 among patients with DSV and 23/785 among patients with non-DSV, and the p value for the difference between these groups was 0.18 by Fisher’s exact test. The cause-specific mortality rate was 1/24 among patients with DSV and 5/767 among patients with non-DSV, with a p value of 0.17 by Fisher’s exact test.
Of the 43 patients with DSV, 39 were alive at the time of the study with a mean survival of 11.1 ± 9.7 years (mean ± SD) after surgery, and 18 of 39 had follow-up for more than 10 years.
The overall incidence of DSV in PTC has been reported to range from 0.1% [7] to 6% [8]. Similarly, Fukushima et al. found that after excluding cases of PMC, the incidence of DSV in PTC was 0.7% [9], which is consistent our result of 0.6%.
The present study confirmed the predominance of DSV among young women [3,10]. However, female predominance is a characteristic finding of PTC in general.
Although DSV is considered a non-tumor forming carcinoma [4],
Carcangiu et al. reported the presence of a tumor-forming type of DSV, in which the tumor-forming type was more predominant than the non-tumor-forming type. They suggested that DSV might begin as a tumor-forming cancer type and change into a non-tumor forming cancer type [3]. In the present study, the macroscopic finding of nodules with clear margins, nodules with blurred margins, and cancers without nodules seems to support this suggestion.
On the disease-free survival period, our follow-up study showed little bit complicated results. Although several interpretations may be possible, we considered that these results were related to wider spread cancer cells in DSV than in non-DSV.
On the mortality, our follow-up study showed that DSV was not a worse prognostic factor than non-DSV. Falvo et al. found that the mortality rate of patients with DSV was higher than the mortality rate of patients with conventional PTC. However, in their study, there was a marked imbalance between the cancer stages of the two groups. Patients with DSV outnumbered patients with conventional PTC in advanced cancer stages, and vice versa in the pT1 stage [11]. In other reports, including the present one, patients who had died of DSV had incomplete excision of the cancer initially and/or had distant metastasis at the initial presentation [9,12]. These reports suggest that the fatality of patients with DSV is not related to the DSV itself but rather to the advanced tumor stage [13] at the initial presentation.
Using the hazard function on data from the SEER Program, Vollmer reported that 56% of fatalities of patients with thyroid carcinoma occur within two years after surgery (rapidly evolving tumor group), and that approximately 80% of tumor-related fatalities occur by 10 years. In his report, PTCs with higher initial stages belonged to the rapidly evolving tumor group [14]. The study by Vollmer also supports the idea that DSV is not an aggressive subtype of PTC. In the present study, the one patient who died of DSV 2 months after surgery had a higher initial cancer stage (stage 4). The other 2 deceased patients who had received radical surgery (this excludes the patient who died in an accident) survived more than 30 years after the surgery. In conclusion, DSV is not an aggressive subtype of PTC and therefore does not require more aggressive therapy than PTC of the same stage.