Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2012) Volume 2, Issue 4
We report a rare case of acinar cell cystadenoma (also called cystic acinar transformation) in a 54-year-old woman who complained persistent and diffuse abdominal pain. Acinar cell cystadenoma it is one of the acinar cell tumors of the pancreas, which also include acinar cell cystadenocarcinomas and acinar cell carcinomas. Acinar cell cystadenoma is considered a benign lesion and no chemotherapy was carried out in our patient. Currently, she is still alive and is being clinically followed as an outpatient.
<Keywords: Acinar cell cystadenoma, Pancreatic neoplasms, Computer tomography
Acinar cell cystadenoma (also called cystic acinar transformation) is a rare pancreatic neoplasm which was described for the first time in 2002 [1]; it is one of the acinar cell tumors of the pancreas, which also include acinar cell cystadenocarcinomas and acinar cell carcinomas [2,3].
In April 2009, a 54-year-old woman complained persistent and diffuse abdominal pain associated with diarrhea; she underwent biochemical examination and abdominal Ultra Sonography (US). The biochemical examination was normal and the US showed a hypoechogenic formation of 10×10 mm in the body-tail of the pancreas. In January 2011, the patient was referred to our Unit for further evaluation. She was a non-drinker and had smoked about 10 cigarettes a day from 18 to 40 years of age. Her past history was unremarkable; however, she continued to complain recurrent abdominal pain, mainly in the postprandial period of 4-6 hours duration. Repeated biochemical examinations were normal as well as fecal elastase 1 determination. Contrast-enhanced Multi Detector Computed Tomography (MDCT) of the abdomen was carried out. The MDCT showed the presence of intraductal non-obstructive calcifications localized at the uncinate process and in the tail of the pancreas (Figure 1a, white arrows); a cystic lesion, 1.4 cm in diameter, was also detected in the body of the pancreas (Figure 1b, white arrow), with a calcification in the posterior wall (Figure 1b, yellow arrow). Endoscopic Ultra Sound (EUS) confirmed the presence and characteristics of the lesion and calcifications of the pancreatic parenchyma. Analysis of the cystic fluid of the cyst showed no malignant cells; in addition, analysis of the cystic fluid revealed amylase levels of 56 U/l and CEA of 4.9 mcg/l. For the presence of recurrent abdominal pain and the suspicion of pancreatic malignancy even if analysis of cystic fluid gave negative results [4], the patient underwent surgery and a laparoscopic spleenpreserving left pancreatectomy was carried out.
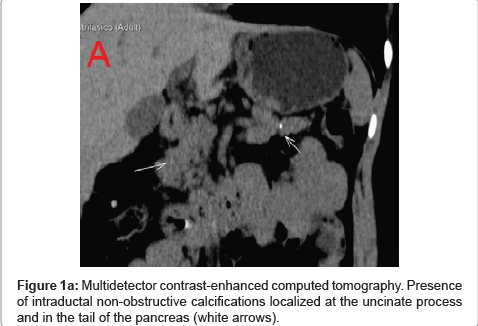
Figure 1a: Multidetector contrast-enhanced computed tomography. Presence of intraductal non-obstructive calcifications localized at the uncinate process and in the tail of the pancreas (white arrows).
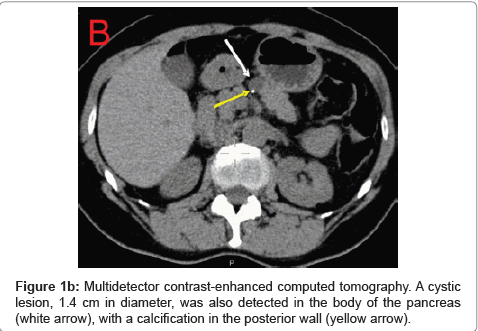
Figure 1b: Multidetector contrast-enhanced computed tomography. A cystic lesion, 1.4 cm in diameter, was also detected in the body of the pancreas (white arrow), with a calcification in the posterior wall (yellow arrow).
Histological examination revealed an acinar cell cystadenoma and chronic pancreatitis (Figure 2). The cyst was lined by a single layer of bland cuboidal or columnar acinar cells with a tendency to crowding; their nuclei were located basally and regular and they contained small nucleoli. The cell cytoplasm was typical of acinar cells. Histochemically, the eosinophilic apical cytoplasm of the cuboidal acinar cells and the acinar cells of the cysts were PASpositive. The acinar cells of the cysts, the acinar structures with cystic transformation and the normal acinar structures were negative for synaptophysin and chromogranin while the normal islet cells were positive for synaptophysin and chromogranin. The acinar cells associated with the cyst epithelium and the normal acinar cells were negative for p53, and their Ki67 index was less than 1%. Finally, acinar cells stain was strongly positive for lipase and amylase [5].
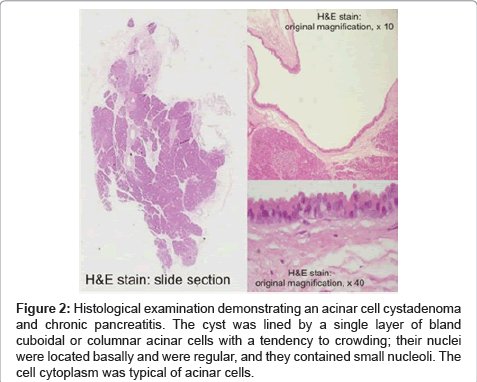
Figure 2: Histological examination demonstrating an acinar cell cystadenoma and chronic pancreatitis. The cyst was lined by a single layer of bland cuboidal or columnar acinar cells with a tendency to crowding; their nuclei were located basally and were regular, and they contained small nucleoli. The cell cytoplasm was typical of acinar cells.
Acinar cell cystadenoma is considered a benign lesion [2] and no chemotherapy was carried out in our patient. Currently, she is still alive and is being clinically followed as an outpatient.
From a clinical point of view, the tumor has been reported mainly in females and the age of diagnosis ranges from 39 to 66 years [3]. The most frequent clinical presentation is acute pancreatitis, but asymptomatic cases, have been reported [3]. The tumor is frequently localized in the head, and multiple localizations in the pancreas have also been reported [3]. The cysts may be uni- or multilocular and a capsule may sometimes be present [3]; size ranges from 0.1 to 10 cm [3]. Ultrasound-guided aspiration of the cystic fluid may be helpful in cases with pancreatic cystic lesions; the levels of amylase are elevated in the cystic fluid of pseudocysts whereas the carcinoembryonic antigen levels may be elevated in mucinous cystic tumors and keratinous and amorphous debris can be found in lymphoepithelial cysts. Considering the rarity of these tumors, there is a lack of data regarding treatment and prognosis.