Journal of Probiotics & Health
Open Access
ISSN: 2329-8901
ISSN: 2329-8901
Research Article - (2017) Volume 5, Issue 4
Objective: Bacillus subtilis probiotics have been shown to influence several aspects of the human gut including motility, epithelial strength, inflammation, etc. that may change bowel movement frequency and/or type. To explore the efficacy of Bacillus subtilis (B. subtilis) DE111 in this regard, 50 people were evaluated by their stool profile, food diary and questionnaire while taking a probiotic or placebo daily over the course of 105-days.
Method: The stools were scored based on the Bristol Stool Chart index and safety was assessed using blood markers during the 0, 45 and 105 days.
Results: Statistically significant results showed those in the DE111 group moved to a healthier bowel index while those in the Placebo group stayed the same.
Conclusion: The study provided evidence that DE111 may improve occasional constipation and/or diarrhea in healthy individuals.
Keywords: Probiotics; Gastrointestinal health; DE111; Bristol stool; Constipation; Diarrhea; Bacillus subtilis
People who have at least one bowel movement per day and pass good textured feces (not too hard or soft) are considered to have ‘normal’ bowel function [1]. However, occasional constipation and/or diarrhea can be a burdensome gastrointestinal issue that occurs in many individuals and whose treatment remains challenging. Some health professionals use the Bristol Stool Chart to classify stool type as it may be difficult to differentiate between normal and abnormal stools [1]. This scale can help assess the consistency and the time stools spent in the bowels. Type 1 stools have spent the longest time, while type 7 stools spend the least time (Figure 1 for the Bristol Stool chart used in this study).
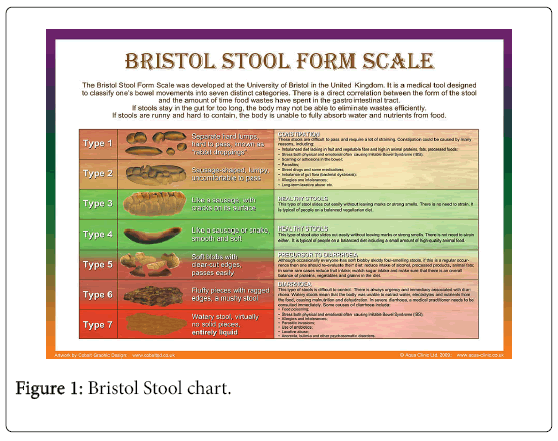
Figure 1: Bristol Stool chart.
People whose stools are classified as type 1 or type 2 are individuals who suffer from constipation. This gastrointestinal discomfort can be the result of many factors including a poor diet, excess stress or the normal aging process. Constipation can often be caused by acute dysbiosis which is common for those that are on antibiotic treatment or low fiber diets. When there is a balance in the normal flora of the gut, beneficial bacteria can hold water facilitating the passing of feces. When absent, the stools lack a normal amorphous quality and become formed lumps which can be hard and abrasive. The typical diameter of these lumps can range from 1 to 2 cm, and can be painful to pass due to their hard and scratchy nature. On the other hand, people who fall within the 5-7 stool range may have a hyperactive colon (fast motility) or excess dietary potassium. These people may suffer from sudden dehydration or stress related spikes in blood pressure; both conditions can cause the rapid release of water and potassium from blood plasma into the intestinal cavity. In addition, stools in this range are indicative of a hypersensitive personality prone to stress, diets rich in spices, fats, high mineral contents and the use of osmotic (mineral salts) laxatives. Probiotic supplementation of the intestinal microflora may promote healthy intestinal homeostasis.
The Bacillus species are rod-shaped, spore-forming, aerobic, grampositive bacteria that are ubiquitous in nature. There is evidence that B. subtilis might be a part of the normal gut flora of humans. Some human intestinal biopsy samples have shown that subtilis does populate the gut in humans as normal human intestinal flora. Bacillus subtilis has been used abundantly in traditional ethnic food processing in East Asia. Natto, in particular, is a cheese-like food, processed by inoculating soaked and steamed soybeans with live Bacillus from rice straw [2,3]. Although the cultural history of B. subtilis fermentation is well known, research on modern uses and consumption of B. subtilis is comparatively very recent. Clinical trials have shown that B. subtilis is safe for consumption, and beneficial for digestive health [4,5].
The term probiotic means “for life” in Greek. It was first used in 1965 by Lilly and Stillwell [4] to name microorganisms that are beneficial to consume. The general health benefits of consuming probiotics have been shown in both animal and human studies. As a component of the human microbiome, Bacillus subtilis has the ability to promote gastrointestinal health, including helping its host in digestion, making it an ideal probiotic.
The purpose of this double-blind, randomized study was to determine the efficacy of B. subtilis DE111 in capsule form for regulation of bowel movements. 50 adults (18-65 years of age at the time of participation) suffering from occasional constipation and/or diarrhea were assigned to consume either 1 × 109 CFU of DE111 or placebo. Each group was instructed to consume one capsule per day with a meal for 90 days. Efficacy was assessed through participantreported bowel movement (BM) records as well as dietary intake logs.
Composition of supplement and placebo
Each DE111 supplement contained a dose of 1 × 109 CFU of B. subtilis DE111 diluted to concentration with low moisture rice dextrin. Placebo supplements contained only low moisture rice dextrin. Both DE111 and placebo were encapsulated in size one opaque vegetable capsules.
Subject recruitment
Participant recruitment included online postings to Clinical Connection, Atlanta Job Exchange, and social media for local interest sites. Furthermore, recruitment flyers were posted throughout the metro Atlanta area.
Participant demographics and inclusion criteria
This study aimed to use a diverse participant population representative of the general population. 50 adults, ages 18-65 at time of participation and suffering from occasional constipation and/or diarrhea completed this study (Initially, 65 individuals were enrolled, 7 were dropped due to their initial blood work results, 6 were dropped due to CRP levels higher than 5 mg/L and 2 opted out mid study). Occasional constipation/diarrhea was defined as frequency ranging from 1-5 episodes per month, with each episode lasting a minimum of 24 hours. Medical history questionnaires, digestive health questionnaires, and initial blood samples were collected and assessed by a board-certified physician to determine general health of participants before complete inclusion [6,7]. Blood samples were also collected at days 45 and 105, and health questionnaires were completed on days 1, 15, 45, 75, and 105. Blood samples were collected at LabCorp locations that were convenient to each participant. C-reactive protein (CRP), lipid panels, and complete metabolic panels (CMP) levels were used as a safety screen to determine participant health at time of inclusion. Trained phlebotomists used routine venipuncture procedures to collect blood samples from participants.
Data collection procedures
Participants recorded daily entries of their dietary intake and BM records throughout the 90 days. The daily BM logs required participants to score their bowel movements using the Bristol Stool chart. Additionally, digestive health questionnaires were completed on days 1, 15, 45, 75 and 105 using the online survey service Survey Monkey. The questionnaires required participants to rate their general digestive health by the following scale: 0=symptom is not present; 1=mild/sometimes;2=moderate/often and 3=severe/almost always. Participants had the option to use controlled electronic documents or hard copy packets to complete the daily BM logs and digestive health questionnaires.
Incentives, follow-ups and compensation
Participants could withdraw from the study at any time without penalty. Daily interaction encouraged participants to maintain daily tasks, ask questions, and voice concerns. Communication included email and phone calls to remind participants of upcoming questionnaires and sample collections. Participants who completed the study were paid an honorarium in appreciation for their time.
Statistical analysis
The participants were tested for differences between the DE111 and the Placebo groups as well as differences within groups. The subgroups included gender female vs male and age, under 30 (n=28) and over 30 (n=22), to preserve a larger sample size and balance proportion between groups (Table 1).
| Demographic | Statistic | Probiotic (A) (N=24) | Placebo (B)(N=26) | Females (36) | Males(N=14) | Under 30(N=28) | Over 30(N=22) | Overall (N=50) |
|---|---|---|---|---|---|---|---|---|
| Age | Mean | 30.1 | 32.9 | 31.5 | 31.9 | 23.3 | 42.6 | 31.6 |
| Min-Max | 19-53 | 22-64 | 19-64 | 20-53 | 19-29 | 30-64 | 19-64 | |
| Bristol Type | Mean | 3.48 | 3.36 | 3.44 | 3.37 | 3.35 | 3.37 | 3.42 |
| Min-Max | 1-7 | 1-7 | 1-7 | 1-7 | 1-7 | 1-7 | 1-7 | |
| *Transit Health | Mean | 3.29 | 3.12 | 3.20 | 3.18 | 3.23 | 3.15 | 3.2 |
| Min-Max | 1-4 | 1-4 | 1-4 | 1-4 | 1-4 | 1-4 | 1-4 |
Table 1: Participant characteristics. *BM health was scaled from the self reported bristol stool types: 1=Very poor; 2=Poor; 3=Failr; 4=Good.
The Bristol stool types describe various states of bowel transit health from hard to pass stools, constipated (Bristol 1-2); normal (Bristol 3-5); and very loose stools, diarrhea (Bristol 6 and 7). This scale was regrouped into a ranking scale starting from 1 (Bristol 1 and 7; the worst scale numbers for diarrhea and constipation), to 2 (Bristol 2 and 6), 3 (Bristol 5) and ideal type 4 (Bristol 3 and 4). Collectively these were referred to as “BM Transit Health”.
Bristol types were placed into a binary categorical group consisting of “Normal” (Bristol 3, 4 and 5) and “Non-normal” stools (Bristol 1, 2, 6, and 7). The data on BM state was divided into six 15 day intervals. Interval 1 (days 1-15), Interval 2 (days 16-30), Interval 3 (days 31-45), Interval 4 (days 46-60), Interval 5 (days 61-75) and Interval 6 (days 76-90). All time groups were tested for independence in proportions using the Chi-Square test statistic.
The proportions between groups and the change in proportions from interval 1 to interval 6 within each group was tested using Chisquared tests for the BM state variable of “normal” and “non-normal” stools. All the hypotheses based tests of proportions were two-sided and statistical significance was accepted at the p=0.05 level. No adjustments for multiple comparisons were made. The questionnaires were analyzed using a paired sample T-Test comparing group scores.
Independent t-tests were used for between group differences with respect to capsule type, and paired t-tests were used to assess within group differences with respect to time. Between group differences with respect to capsule type are reported. Independent samples T-tests were used to test for differences between Capsule A and Capsule B at each point of the study, baseline, mid and final. Paired samples t-tests were used to assess the differences between Capsule A at baseline, mid-point and post study; and for Capsule B at each point in the study. P-values below 0.05 were considered significant, and p-values between 0.05-0.10 were considered near significant.
All statistical analysis was completed using the R language and environment for statistical computing (version 3.3.2, R Foundation for Statistical Computing, Vienna, Austria).
The mean BM Transit Health was significantly different in days 75-90 (last two weeks) vs the first two weeks among the Capsule A group (p-value=0.0369) moving from non-healthy stools to healthy stools. There were no strong differences found when other ranges of days were compared in the placebo group (Table 2).
| Day 1-15 | Day 75-90 | P - Value | ||
|---|---|---|---|---|
| Capsule A | Mean | 3.29 | 3.45 | 0.369 |
| Capsule B | Mean | 3.06 | 3.08 | 0.7386 |
Table 2: Mean BM Transit Health for Days 1-15 vs. Days 75-90.
Comprehensive metabolic panels and lipid panels stayed within normal reference ranges both in the probiotic and placebo groups with no adverse effects or significant serum level differences. CRP levels remained within normal levels for both probiotic and placebo groups throughout the study.
The results of the Chi-Square test indicated that over time and by Interval 6, the strength of the difference in proportions of normal vs non-normal stool types increased for the probiotic group (Figure 2).
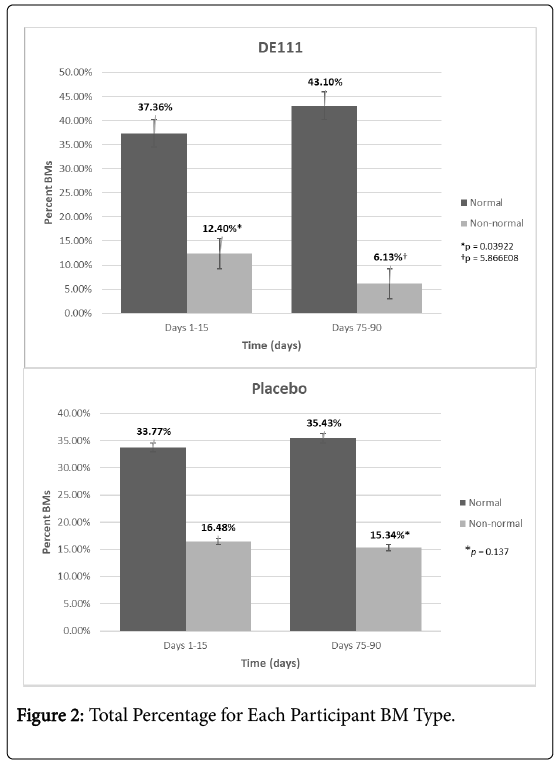
Figure 2: Total percentage for each participant BM Type.
The difference in means between Interval 1 and Interval 6 for the DE111 are statistically significant. By day 90 the proportion of normal stools (43.1%) to non-normal stools (6.13%) in the DE111 group differed significantly (p=5.866E-08; Chi-squared 29.407) from that in the Placebo group (Figure 2 and Table 3). The proportion of normal Bristol stools type 3 and 4 increased from 37.36% in week 1 to 43.1% in the last week of the study. The proportions of normal stools in the Placebo group stayed roughly the same from 33.77% to 35.43%, the degree of change was insignificant and not attributable to any other factor in the research (p=0.137; Chi-squared 2.204). By days 75-90, there is a significant increase in normal stool types of participants in DE111 group. This was not observed in the placebo group which actually showed a decrease in normal stools.
| Interval | A | B | Group Total | Chi-Square | P-Value | |
|---|---|---|---|---|---|---|
| Non-normal | 1 | 76 | 101 | 177 | 4.2511 | 0.03922 |
| Normal | 229 | 207 | 436 | |||
| Non-normal | 2 | 68 | 105 | 173 | 9.0109 | 0.002684 |
| Normal | 235 | 207 | 442 | |||
| Non-normal | 3 | 64 | 85 | 149 | 2.6626 | 0.1027 |
| Normal | 237 | 227 | 464 | |||
| Non-normal | 4 | 70 | 97 | 167 | 3.4943 | 0.06158 |
| Normal | 235 | 228 | 463 | |||
| Non-normal | 5 | 71 | 111 | 182 | 9.7593 | 0.001784 |
| Normal | 238 | 210 | 448 | |||
| Non-normal | 6 | 40 | 100 | 140 | 29.407 | 5.87E-08 |
| Normal | 281 | 231 | 512 |
Table 3: BM state compared by capsule group, time and range.
Results of the questionnaires completed were analyzed. Paired sample t-tests of groups showed a reduction in the mean score for the question “Have you experienced alternating constipation and diarrhea?” (0=symptom is not present, 1=sometimes, 2=often, 3=almost always) from a day 1 mean of 0.42 down to a day 15 mean of 0.11 (p=0.05). No other statistically meaningful differences between the DE111 and Placebo groups or between questions were found.
Bacteria make up more than 50% of the composition of a healthy person’s stool and play a major role in the quality and frequency of bowel movements. Probiotics are live microorganism that confer a gastrointestinal health benefit to the host. Gastrointestinal regularity may be the result of several potential probiotic mechanisms of action. The presence of probiotics may modify the gastrointestinal microbiota. This beneficial bacteria may release metabolites that can alter gut function, including satiety and motility. Some probiotics can increase the production of lactate and short-chain fatty acids, reducing luminal pH, which has been proposed to enhance gut transit time and reduce inflammation.
DE111 significantly improved gastrointestinal discomfort including constipation and diarrhea over the course of the study. Individuals in the DE111 group reported an increased frequency of normal type stools compared to those in the Placebo group. Therefore, a B. subtilis DE111 dose at 1 billion CFU/day may improve occasional constipation and diarrhea while helping to maintain gastrointestinal health.
We would like to thank Judy Brumlow for providing writing and editing assistance, Jon Starnes for technical help and Sonaina Khan for general support and contributions to our research.
Supported by Deerland Enzymes
The author(s) of this publication had research support from Deerland Enzymes.