Journal of Probiotics & Health
Open Access
ISSN: 2329-8901
ISSN: 2329-8901
Research Article - (2015) Volume 3, Issue 2
Background: Current guidelines recommend first line triple treatment with PPI-clarithromycin and amoxicillin or metronidazole with efficacy of these regimes approaching 70%. Adding a probiotic is a possible means to increase the eradication rate.
Aim: To determine whether treatment with L. reuteri ProGastria+PPI is effective in eradicating H. pylori alone or facilitating subsequent eradication.
Methods: A randomized, double-blind, placebo-controlled clinical trial performed in a tertiary care setting. A total of 55 patients with dyspeptic symptoms were tested for H. pylori infection by 13C-UBT, stool antigen test, histology and rapid urease test and randomly allocated to omeprazole (2 × 20 mg/day)+placebo or probiotic for 28 days. Afterwards a stool antigen test was performed and if positive a sequential regimen was prescribed. At the end UBT and stool antigen test were performed. A gastrointestinal symptom rating score was completed at baseline, Day 14, 28 and 90.
Results: At the end of treatment 57.7% of the patients from the probiotic group and 62.1% from the placebo group had positive stool antigen test (p=0.75, Pearson`s correlation test). Twenty patients were prescribed sequential therapy. Unsuccessful eradication was present in 27.2% from the probiotic group versus 55.6% from the placebo (p=0.36, Fisher`s exact test). A trend towards a lower mean symptom score for the patients treated with probiotic was noted (p>0.05).
Conclusion: Although the lacking an ability of ProGastria to eradicate H. pylori, the study showed a trend towards a higher rate of successful eradication if sequential regimen was preceded by a 28-day probiotic treatment.
Keywords: H. pylori; Eradication; Sequential treatment; Probiotics; L. reuteri
H. pylori (HP) is one of the most commonly diagnosed pathogens in humans affecting more than 50% of the global population [1]. The estimated prevalence of HP infection in the developed European countries is between 10 and 30% with an increase of 1-3% for each year decade, while more than 95% of the population in the developing regions is believed to be HP positive [2]. In Bulgaria as part of Eastern Europe HP infection is found in 78.3% of the symptomatic elderly population [3] and in 61.7% of children with gastroduodenal diseases [4]. More detailed data from our northern neighbor–Romania, show overall prevalence of HP infection in 68.5% of the adult population with slight preponderance in males [5].
HP infection is acquired early in childhood and is associated with dyspepsia, chronic gastritis, intestinal metaplasia, peptic ulcer disease, Mucosa-Associated Lymphoid Tissue (MALT) lymphoma and gastric cancer. Also, there is evidence that links HP with some extragastric conditions such as iron-deficiency anemia, idiopathic thrombocytopenic purpura, and vitamin B12 deficiency [1]. Hence, successful eradication of HP infection is expected to cure and/or protect from recurrence of the above mentioned conditions. Current evidence-based guidelines recommend first line triple treatment including PPI-clarithromycin and amoxicillin or metronidazole [6]. However, recent data have shown that the efficacy of these regimes has dropped to 70% successful eradication [7], the main reasons for this being attributed to compliance, high gastric acidity, high bacterial load, type of strains but most importantly to resistance to clarithromycin. Possible ways to overcome the increasing rate of unsuccessful eradications are: sequential treatment, quadruple therapy, antibiotic susceptibility testing, extension of treatment duration to 10-14 days, or even adding a probiotic [1].
Recent observations have proven that dietary supplementation with the probiotic L. reuteri in humans leads to colonization of the human gastric epithelium [8,9] and inhibition of the growth of H. pylori [10]. L. reuteri is one species of lactobacillus that naturally inhabits the gastrointestinal tract of humans [11] and numerous studies have found it safe for human consumption [8,12]. Studies using supplementation with L. reuteri in both symptomatic and non-symptomatic H. pylori-infected subjects show a clear reduction of infection load after 4 weeks of use and reduction in symptoms associated with the infection [13,14]. Further, dietary supplementation with L. reuteri during and after the period of H. pylori eradication therapy has also been shown to reduce the side effects of this therapy without affecting the degree of eradication [15-17]. When 2 × 108 CFU L. reuteri ATCC 55730 was given to symptomatic H. pylori-infected patients together with 2 × 20 mg omeprazole alone for 30 days, there was an apparent eradication of the infection in 9 of 15 subjects [18]. Recent unpublished data from open clinical observational studies in Slovakia have shown that in more than 55% of H. pylori-infected patients showed loss of their infection when given 2 × 108 CFU L. reuteri ATCC 55730+2 × 20 mg omeprazole for 28 days. Thus, there is good reason to believe that giving L. reuteri strains together with proton pump inhibitors (PPI) in the absence of antibiotics, may eradicate H. pylori infection at least in 50% of the treated patients.
The primary objective of this study was to determine whether dietary supplementation with L. reuteri ProGastria (a combination of L. reuteri DSM 17938 (formerly ATCC 55730) and L. reuteri ATCC PTA 6475) is effective in controlling infection loads in H. pylori-infected subjects when given PPI in the absence of antibiotics. The secondary objective was to assess the effect of the probiotic on the subsequent eradication rate in those patients who were positive for HP after the initial supplementation with L. reuteri.
Participants: Consecutive subjects, aged 18–70 years with dyspeptic symptoms not previously treated for H. pylori infection, which were referred to our academic tertiary health care center for consultation, were considered eligible. Key exclusion criteria were duodenal or gastric ulcer, MALT lymphoma, previous gastric resection, first level relatives of gastric cancer patients, use of non-steroid anti-inflammatory drugs (NSAIDs), aspirin or other anti-inflammatory drugs within 1 week (for occasional use) or 3 weeks (for chronic use) of inclusion and use of oral antibiotics and/or PPIs and/or H2-antagonists during the 2 weeks prior to ingestion of the study product.
Trial design: This was a randomized, double-blinded, placebo-controlled parallel clinical trial. After signing an informed consent patients were tested for presence of H. pylori by 13C-urea breath test (13C-UBT), stool antigen test, and by histology and rapid urease test from samples obtained from upper endoscopy. The latter was used also to exclude peptic ulcer disease and neoplasia. Those patients who were found positive for at least one test were randomly assigned in a 1:1 ratio to either omeprazole (2 × 20 mg/day)+1 tablet placebo per day or omeprazole (2 × 20 mg/day)+1 tablet (2 × 108 CFU L. reuteri) ProGastria per day. Both patients and investigators were blinded to the allocated treatment. Intervention began on Day 1 and lasted for 28 days after which therapy was stopped. One week after treatment discontinuation all patients were tested for H. pylori infection using the stool antigen test. If H. pylori infection was confirmed, these subjects were given sequential therapy to eradicate the infection and followed up until Day 90 of the study. The sequential therapy comprised Pantoprazole 2 × 40 mg/day plus Amoxicillin 2 × 1 g/day for the first 5 days followed by Pantoprazole 2 × 40 mg/day plus Metronidazole 2 × 500 mg/day plus Clarithromycin 2 × 500 mg/day for the next 5 days. On Day 90 UBT and stool antigen test were again performed to determine the presence of H. pylori infection. During the period of the study all subjects refrained from ingestion of any kind of probiotic, other bacterial preparation, antibiotics, H2-antagonists, other PPIs and NSAIDs.
Sample size: Based on data presented by Saggioro et al. [18] and an open unpublished trial performed in Slovakia in 2009, it was expected that elimination of the infection will be seen in 50% of the subjects given ProGastria compared to none in the placebo group. The total number of subjects needed to achieve 90% power to get a difference at the 5% level (P<0.05, two-sided hypothesis) and detect a difference in of 40% in the test group compared to 1% in the placebo group is 46, 23 subjects per arm. To allow for attrition, an extra 5 subjects per arm were included. Thus, 56 subjects were randomized, 28 in each arm.
Questionnaire: After randomization on Day 0 of the study, the subjects were asked to complete a gastrointestinal symptom rating score (GSRS) to determine baseline symptomology. The latter was completed also on Day 14, Day 28 and on Day 90 at the end of the study. The questionnaire included information regarding presence of abdominal pain, acid regurgitations, nausea, vomiting, abdominal distention, belching, flatulence and change in bowel habits. Each symptom in every patient was assessed using a scoring system ranging from 0 to 3 with 0 representing absence of a symptom and 3–most severe expression of the symptom. For each visit an average symptom score was calculated as a sum of scores of all symptoms divided by the number of symptoms.
Tests for evaluation of H. pylori infection: The presence of H. pylori infection was assessed simultaneously by 4 methods: stool antigen test, 13C-urea breath test, histology and rapid urease test. One fecal sample per patient per visit was sent to a validated laboratory which performed an ELISA-test using monoclonal antibodies (BioGaia PPL®). If stool sample was obtained the previous day, an overnight storage in the refrigerator by 4°C was advised. Urea breath tests were performed in the morning after overnight fasting by means of 13C-urea breath test. Initially patients were asked to exhale air in two 20-ml vacutainers using a straw. A test drink containing citric acid solution (1 g dissolved in 180 mL of still water) followed by dissolved 75 mg of 13C-urea (Helicobacter Test INFAI, INFAI GmbH, Köln, Germany) were ingested consecutively. After 30 min breath samples were collected in two 20-mL vacutainers using a straw. Tubes with breath samples were sent for mass spectrometry (IRMS) per post. The method analyzed the ratio between isotopes 13C and 12C. Samples with difference in 13C/12C ratio at initiation and after 30 min exceeding 4% were considered positive for H. pylori infection.
Upper endoscopy using Olympus Exera II workstation and gastroscope Olympus GIF-Q180 was performed in every patient for excluding major pathology such as peptic ulcer disease or gastric cancer. During upper endoscopy 5 samples per patient were obtained: 3 from the antral region and 2 from the corpus. One from the mentioned biopsies from the antrum was used for rapid urease test. The remaining 4 biopsies were fixed in formalin and sent to a validated pathological laboratory for histological analysis. Samples were embedded in paraffin and stained in H&E for assessment of glandular structure and inflammation, and in Giemsa for presence of H. pylori.
The primary endpoint of the study was the HP eradication rate of L. reuteri versus placebo both in combination with PPI. Secondary endpoints were the ability of ProGastria to maintain the absence of H. pylori infection up to 2 months after completed treatment, to ameliorate gastrointestinal symptoms in H. pylori-infected subjects compared to PPI alone and to improve eradication rates of H. pylori using triple therapy.
Ethical approval: The study was approved by the University Hospital Ethical Committee. After explaining the details of the protocol all patients received written informed consent about the project and signed it.
Statistical analysis
Data were analyzed with computer software SPSS 17 v 1.0. The statistical significance of all statistical tests was performed at the 5% level of significance. The unpaired Student’s t-test was used to compare means of continuous variables approximating a normal distribution and Mann-Whitney U-test for variables with other types of distribution. Proportions were compared by using χ² test or Fisher’s exact test with calculating odds ratio and 95% confidence intervals. The difference between groups was considered significant at p<0.05.
Between May 1, 2011 and May 1, 2012 a total of 59 patients were found eligible for the study. Four patients were excluded initially–3 due to unconfirmed infection with HP and 1 due to a positive familial history for gastric cancer. A flow diagram of progression is shown in Figure 1. In total 55 patients were randomized to either omeprazole (2 × 20 mg/day)+1 tablet placebo per day or omeprazole (2 × 20 mg/day)+1 tablet ProGastria per day. The mean age of the study population was 48.3 ± 14.3 years. Of them 50.9% (28/55) were female and 49.1% (27/55) were male. Baseline characteristics of the participants are presented in Table 1.
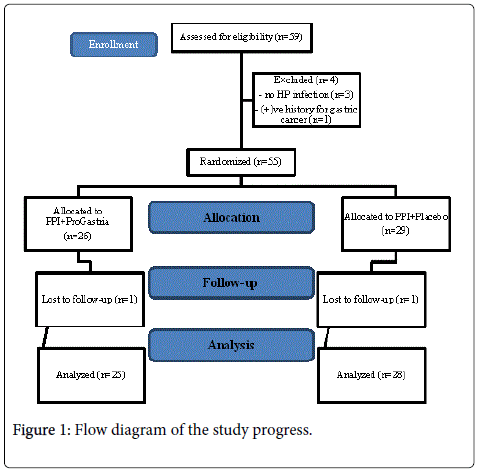
Figure 1: Flow diagram of the study progress.
| ProGastria (n=26) | Placebo (n=29) | p | |
|---|---|---|---|
| Age (mean ± SD) years* | 49.0 ± 14.5 | 47.7 ± 14.3 | 0.73* |
| Sex Male Female |
15 (57.7%) 11 (42.3%) |
11 (37.9%) 18 (62.1%) |
0.23§ |
| BMI* | 27.9 ± 6.3 | 26.2 ± 4.7 | 0.26* |
| Positive stool antigen test | 22 (84.6%) | 24 (82.8%) | 0.58§ |
| Positive UBT | 21 (80.8%) | 23 (79.3%) | 0.42§ |
| Positive histology | 19 (73.1%) | 20 (68.9%) | 0.47§ |
| Positive rapid urease test | 20 (76.9%) | 24 (82.8%) | 0.59§ |
Table 1: Baseline characteristics of the patients. *Unpaired Student’s ttest; §χ2-test.
There were no differences between placebo and on treatment group regarding baseline characteristics such as age, sex and BMI (p>0.05). Also, no difference between the percentage of patients with positive stool antigen test, 13C-UBT, histology or rapid urease test between placebo and study medication group were observed (p>0,05). Of note, 11.5% (3/26) of the ProGastria group and of the 10.3% (3/29) placebo group were found positive for only stool antigen test and negative for the remaining 3 tests. As expected, the difference was not statistically significant (p>0.05).
On Day 36, one week after treatment discontinuation, patients were tested for presence of H. pylori infection by means of stool antigen test. Negative stool antigen test was found in 57.7% (15/26) of the patients from the ProGastria group and in 62.1% (18/29) from the placebo group (p=0.75, Pearson`s correlation test). The remaining patients from both groups were prescribed sequential eradication therapy for 10 days.
Two patients were lost to follow-up, therefore on Day 90 53 patients were tested for presence of H. pylori infection by means of stool antigen test and UBT. The analysis included all patients irrespective of their H. pylori status on Day 36. No statistical differences between the two groups were found (Table 2). Surprisingly, a large difference in the proportion of patients with positive UBT and stool antigen test on Day 90 was noted (Figure 1). Although not reaching statistical significance, patients from the ProGastria group had a lower rate of positive stool antigen test than the placebo group (Table 2).
| ProGastria (n=11) | Placebo (n=9) | OR | 95% CI | p§ | |
|---|---|---|---|---|---|
| Positive stool antigen test | 4 (36.4%) | 2 (22.2%) | 2.0 | 0.27-14.7 | 0.64 |
| Positive UBT | 3 (27.2%) | 5 (55.6%) | 0.3 | 0.04-1.94 | 0.36 |
Table 2: Percentage of patients with positive UBT and stool antigen test on Day 90. §Fisher’s exact test; *χ2-test; CI–confidence intervals.
We also checked whether treatment with ProGastria could modify the effect of the subsequent eradication with PPI and antibiotics. From the 20 patients who were prescribed sequential therapy 60.0% (12/20) had successfully eradicated H. pylori according to the UBT result and 70.0% (14/20) had negative stool antigen test. Patients who received initial probiotic treatment with ProGastria had lower rate of unsuccessful eradication (27.2% (3/11)) than those who were treated with placebo (55.6% (5/9)). However, the results did not reach statistical significance (Table 3). Again, a discrepancy between the results from the UBT and stool antigen test was present.
| ProGastria (n=11) | Placebo (n=9) | OR | 95% CI | p§ | |
|---|---|---|---|---|---|
| Positive stool antigen test | 4 (36.4%) | 2 (22.2%) | 2.0 | 0.27-14.7 | 0.64 |
| Positive UBT | 3 (27.2%) | 5 (55.6%) | 0.3 | 0.04-1.94 | 0.36 |
Table 3: Percentage of patients with unsuccessful eradication on Day 90. §Fisher’s exact test; CI–confidence intervals.
In order to minimize the discrepancy between the ability of stool antigen test and UBT to detect presence of H. pylori infection and the higher sensitivity and specificity of UBT, we decided to exclude patients with initially negative UBT. From the 20 patients who performed sequential eradication 1 patient from the ProGastria was excluded from the analysis. On Day 90 the proportion of patients who received initial treatment with probiotic and had unsuccessful eradication was lower than those who were treated with placebo–33.3% (4/12) vs. 71.4% (5/7). Unfortunately, this did not reach statistical significance (OR 0.2 (95% CI 0.03-1.5) p=0.17, Fisher`s exact test).
Interestingly, from the 30 patients who were stool antigen test negative on Day 36 (16 from the placebo group and 14 from the on treatment group) 10% (3/30) had eventually positive stool antigen test on Day 90. All of them had positive UBT as well. Of them 7% (1/14) were treated with ProGastria and 12.5% (2/16) with placebo. No difference between the studied groups was observed (OR 0.58 (95% CI 0.05-7.11) p=1.0, Fisher`s exact test).
Regarding the symptom analysis a trend towards a lower mean symptom score for the patients from the ProGastria group was noted. However, this did not reach statistical significance (Table 4).
| Total GSRS score | N | Mean | Std. deviation | Std. error mean | p | 95% Confidence Interval of the Difference | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Visit 1Placebo ProGastria |
12,34 10,31 |
5,009 6,272 |
0,930 1,230 |
0,19 | -1,018 | 5,093 | |
| Visit 2Placebo ProGastria |
7,21 5,08 |
4,647 4,098 |
0,863 0,804 |
0,08 | -,252 | 4,512 | |
| Visit 3Placebo ProGastria |
3,79 3,32 |
2,908 3,351 |
0,540 0,670 |
0,58 | -1,236 | 2,182 | |
| Visit 4Placebo ProGastria |
2,27 2,23 |
3,144 3,141 |
0,617 0,616 |
0,96 | -1,712 | 1,789 | |
Table 4: Gastrointestinal symptom rating score at baseline, 2nd, 3rd and 4th visits. t-test.
In this prospective, randomized, double-blind, placebo-controlled study we failed to show a superiority of the probiotic treatment with PPI over placebo for eradicating HP after 28 days of treatment. There was a clear trend towards higher eradication of HP with sequential quadruple therapy in patients who were initially treated with ProGastria compared to placebo but the results did not reach the desired level of statistical significance.
According to our baseline data we noticed a discrepancy regarding the rate of positivity of the four diagnostic tests for HP infection. The highest positivity was observed for the stool antigen test and the lowest for the invasive histology and rapid urease tests. This is not surprising since HP shows patchy colonization and thus the appropriate region may not have been biopsied. More importantly, 10% of the patients from both placebo and on treatment groups were found positive for stool antigen test only. According to the Maastricht IV criteria from 2012 the diagnostic accuracy of the stool antigen test and 13C-UBT are equivalent provided that a monoclonal test is used [1]. We used a validated laboratory which implemented a monoclonal antibody test especially for our analyses. Therefore, the apprehension of using inappropriate method with low diagnostic yield is eliminated. One possible explanation for these discrepancies is that some patients might not have fasted before the UBT and that we have not biopsied the colonized mucosal region. Other studies have also shown 10-40% false negative results for 13C-UBT which can be attributed to treatment with PPI and H2-antagonists [19,20]. Since all of our patients had dyspeptic symptoms some of them may have not have shared that they were on such antisecretory treatment when they were tested. Therefore, we support the notion that at least two non-invasive tests or at least one non-invasive and one invasive test should be performed for adequate diagnosis of HP infection.
After 4 weeks of treatment with PPI+ProGastria or placebo 57.7% of the patients from the former group and 62.1% from the latter group had negative stool antigen test, which is statistically insignificant (p=0.75, Pearson`s correlation test). It seems that PPI+probiotics alone are unable to suppress H. pylori according to our results. In contrast to our study Dore et al. proved eradication in 14.2% of patients treated with PPI+L. reuteri but the treatment period was twice as long as ours [21] while Navaro-Rodrigez T et al. found no increase in efficacy or decreases the adverse effects of the treatment with a probiotic compound compared to placebo [22]. The issue of anti-HP activity of probiotics is known and investigated in several in vitro studies. This has been associated with competing with HP adhesins, stimulating mucin production, secreting bacteriocins, lactic, acetic acids and hydrogen peroxide which lead to decrease in HP urease activity, and interacting with epithelial cells and modulating anti-inflammatory cytokines [23]. Nevertheless, eradication of HP has been rarely documented [23,24]. Boyanova et al. have studied the effect of the well-known Bulgarian probiotics Lactobacillus delbrueckii subsp. bulgaricus and Streptococcus thermophilus on HP clinical isolates in vitro and has proven their inhibitory properties but at low pH levels [25]. Hence, withholding from adding a PPI to a treatment with probiotic is a possible way of increasing its effectiveness.
Another possible explanation for the lack of effectiveness of our treatment regime with ProGastria could be the early testing with stool antigen test–only one week after PPI discontinuation. According to the Maastricht IV guidelines PPI should be stopped for 2 weeks before testing by culture, histology, rapid urease test, 13C-UBT or stool test and this period allows repopulation of bacteria in the stomach and restoring the positivity of previously negative tests [1]. However, our results showed that only three patients (10%) resumed their stool antigen testf positivity during the 8 weeks of follow-up. This fact shows that one week is a suitable period for checking for the presence of HP after treatment discontinuation.
One drawback of our study is that we did not perform a UBT test on day 36. If the results from this highly sensitive test were concordant with the negative ones from the stool antigen test, this could mean that treatment successfully eradicated the HP infection. However, if the results were discordant (the negative stool antigen test was accompanied by positive UBT) this could mean that therapy effectively suppressed HP colonization of the gastric mucosa beyond the sensitivity of stool antigen test and that UBT would be more sensitive for following-up of treated patients.
The overall eradication rate of the sequential regimen among our studied population is 60% which is lower than expected. Data from two meta-analyses from Asia and Europe showed 87.6% and 84.3% eradication rate of sequential therapy, respectively [26,27], and a single-center study from Turkey which neighbors Bulgaria reported a 71.4% rate of successful treatment [28]. Patients` compliance is an important issue and should always be considered when treatment period exceeds one week and when the medications` switch relies on patients themselves. On the other hand, antibiotic resistance should not be underestimated. Primary clarithromycin resistance for Europe is reaching 17.6% [29], for metronidazole it is 26%, while for amoxicillin is below 1% [30]. Data from a national study analyzing the prevalence of multidrug-resistant H. pylori in Bulgaria showed that resistance to clarithromycin, metronidazole and amoxicillin was 18.4%, 26.5% and 4.4%, respectively. Strains, resistant to both clarithromycin and metronidazole were found only in 8.0% of the cases [31]. Therefore, the fact that the eradication rate of the sequential treatment regimen among our patients is lower than in Europe and Asia and closer to Turkey could be attributed to a local selection of a different bacterial strain that shows slightly higher resistance to clarithromycin and amoxicillin. Macrolides are one of the most frequent antimicrobials used for treatment of upper respiratory tract infections in children and data show that sequential therapy is able to eradicate as much as 72.5% of strains resistant to clarithromycin [27].
One of the main findings in our study was that compared to placebo more patients treated for 28 days with ProGastria achieved successful eradication with 10-day sequential therapy afterwards-33.3% vs 71.4%, respectively. Unfortunately, this did not reach statistical significance (p=0.17, Fisher`s exact test). Recent data, mostly from Asia, support our results. In their meta-analyses Zheng X, et al. and Wang X et al. proved that lactobacillus-containing probiotics as an adjunct improved eradication rates and reduced the total incidence of side effects of eradication schemes [32,33]. This phenomenon could be explained by the durable colonization of L. reuteri in the gastric mucosa and the exerted antagonism towards HP which probably aids the subsequent eradication. We believe that the lack of statistical significance of our results can be attributed to the low number of patients since only 20 persons were found positive for HP after 4 weeks of treatment with ProGastria and were prescribed eradication. Although the lack of evidence for effectiveness probiotics should be added to standard treatment regimes in order to reduce side effects and one of the main concerns is that long term use of both PPIs and antibiotics are associated with Cl. difficile colitis.
In conclusion, our study showed that treatment with PPI+probiotic is ineffective in eradicating H. pylori infection in adults. A clear trend towards better eradication was observed if patients were treated with probiotic for four weeks prior to initiation of sequential 10-day regimen.