Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Review Article - (2013) Volume 1, Issue 2
Introduction: Several reports have shown a positive correlation between parity and Bone Mineral Density (BMD) and a reduced hip fracture rate, although other studies have reported either no correlation between parity and Bone Mineral Density (BMD) or a negative correlation in postmenopausal women. Hence, a systematic review is needed to help clarify these discrepancies and determine the effect of parity on bone mineral density.
Objective: This study was designed to examine the effect of parity on bone mineral density in postmenopausal women.
Methodology: A systematic review of 19 published studies reporting the effect of parity on bone mineral density of 27,434 nulliparous and parous post menopausal women was conducted and a narrative analysis was made. A total of 356 articles were initially browsed (205 from Pub MED/Medline, 61 from HINARI, and 90 from Google scholar). All English titles and abstracts were scanned to eliminate duplicates and to assess for relevance. Additional references were found through bibliographic searches of all retrieved articles. Studies were included if they (a) examined effect of parity on BMD (by absorptiometry or quantitative ultrasound), (b) included post menopausal women.
Result: Out of nineteen studies eight of them, 1 cohort, 1 case control, and four comparative cross sectional studies, with a combined total of 17,077 subjects concluded that parity positively influences bone mineral density. In contrast to the papers who reported positive effects, six studies; 1 retrospective record review, 1 case control, and 6 comparative cross sectional with a combined total of 7,410 subjects concluded that there is a negative effect of parity on bone mineral density in the post menopausal women. Five comparative cross sectional studies with a combined total of 2,947 women reported that there is no effect of parity on bone mineral density in post menopausal women.
Conclusion and recommendations: The majority of the studies supports a positive effect of parity on BMD in postmenopausal women (with a combined total of 17,077 subjects), while, six studies support a negative effect of parity on BMD (with a combined total of 7,410 subjects). Furthermore five studies (of 2,947 women) did not find any effect. Because most of the studies found were of generally lower level evidence it was difficult to make firm conclusions. Hence, further robust, well designed observational studies should be carried out to confirm these results. Ideally, any future studies would also take into account for the consistent measurement and standardization of DEXA/QUS sites and categorization of parities.
<Keywords: Parity; Post menopausal women
BMD: Bone Mineral Density; DEXA: Dual Energy Absorptiometry; QUS: Quantitative Ultrasound
Bone tissue continues to renew itself, or remodel, throughout life by breaking down old bone (bone resorption) and replacing it with new bone (bone formation). Because lifestyle changes made during the acquisition phase affect the achievement of peak bone mass, these lifestyle changes are critically important to bone health throughout life.
Adolescence is a particularly critical period for bone health because the amount of bone mineral gained during this period typically equals the amount lost throughout the remainder of adult life. Failure to achieve an optimized bone masses at the end of adolescence leaves an individual with much less reserve to withstand the normal losses during later life. Most gains in bone mass during puberty are due to an increase in bone length and size rather than bone density [1]. Fracture rates go up during this period of extremely rapid growth, possibly because the bone is temporarily weaker because bone mineralization lags behind growth in bone length [2].
Individuals achieve peak bone mass in late adolescence, bone health is optimized by maintaining as much of this bone mass as possible throughout adulthood. Bone formation and resorption are generally in balance with each other during the young to mid-adult years, so optimal bone mass is maintained at many skeletal sites. There is bone loss at some skeletal sites, such as the hip, before age 50, but it does not normally compromise strength. Bone loss begins or accelerates at midlife for both men and women, meaning that the goal during this time of life is to keep bone loss to a minimum and to recognize and avoid both bone-specific and non-specific threats to bone health, such as other illnesses and falls. After age 40-50, bone loss may progress slowly in both sexes, with a period of more rapid loss in women surrounding the menopausal transition [3].
| S. No | Data base | Search terms/key words | Hits/articles |
|---|---|---|---|
| 1 | Pubmed/MEDLINE | Parity and bone mineral density or bone mineral content or bone mass in post menopausal women | 205 |
| 2 | HINARI/SCIRUS | Parity and bone mineral density or bone mineral content or bone mass in post menopausal women | 61 |
| 3 | Google scholar | Parity and bone mineral density or bone mineral content or bone mass in post menopausal women | 90 |
| Total | 356 | ||
Table 1: Summary of hits from electronic search engines.
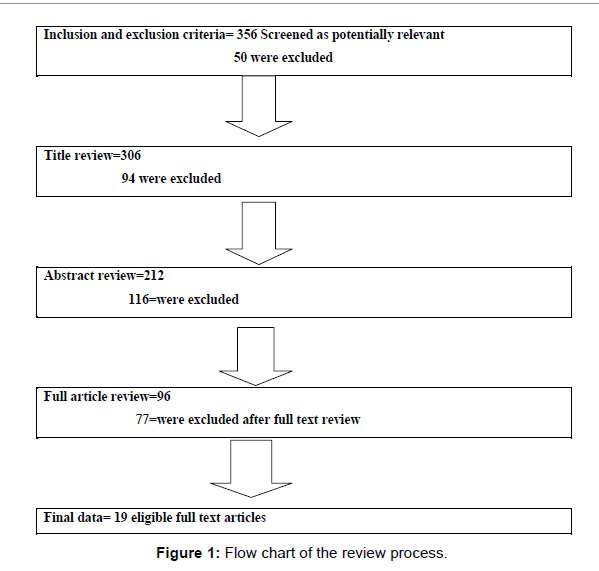
Figure 1:Flow chart of the review process.
Research suggests that a well-balanced diet is important for bone health throughout life. Depending on age, it may help increase or preserve bone mass. Much of the research to date has focused on calcium and vitamin D. Calcium and vitamin D play crucial roles in bone health, although other nutrients are also important. Reproductive hormones play a central role in BMD levels among both women and men, but these hormones have been most widely evaluated in young to middle-aged women, particularly with respect to pregnancy, lactation, and contraception.
Several changes occur during pregnancy and lactation that can affect bone mass, including changes in reproductive hormones and in hormones that affect calcium metabolism. Since fetal and infant bone growth during pregnancy and lactation depends on calcium transfer from the mother, the possibility that pregnancy and lactation affect risk for bone mineral loss later in life has been investigated. Intestinal calcium absorption increases during pregnancy to meet many of the fetal calcium needs, but maternal bone losses may occur in the last months of pregnancy [4]. The mother’s skeleton also loses bone during breastfeeding, but this loss is largely restored during weaning, as ovulation and menses are re-established. This bone loss and its subsequent restoration appear to be independent of lifestyle behaviors, including dietary calcium intake and physical activity patterns [5].
Vis-à-vis epidemiologic studies indicate that neither extended lactation nor multiple pregnancies are associated with subsequent osteoporosis, whether measured by BMD levels or by assessment of fracture risk [6]. In contrast some studies report, the risk of hip fracture in women has been found to decrease by 5-10 percent with each additional child, and there is no apparent association between the duration of lactation and fracture risk [7]. In the same line some researchers’ belief that, pregnancy and lactation in healthy adult women do not appear to cause lasting harm to the skeleton. For example, in one recent study, women with more than 10 pregnancies and extended lactation had BMD levels similar to those in women who have not been pregnant [8]. Having more children also does not appear to increase fracture risk [9]. For pregnant teens that have not yet reached peak bone mass, the 30 g of calcium required for the fetal skeleton competes with the demands of calcium for the teen’s mineral accrual. Whether peak bone mass is compromised in women who experience teen pregnancies remains controversial [10].
Several reports have shown a positive correlation between parity and Bone Mineral Density (BMD) and a reduced hip fracture rate, while other studies have reported either no correlation between parity and Bone Mineral Density (BMD) or a negative correlation. Many of the studies of this issue have been performed in premenopausal women or in women younger than the age typically seen for osteoporotic fracture. In addition, many studies have been conducted on women with low (e.g. 1-3) parity. The few studies of parity and Bone Mineral Density (BMD) conducted in relatively high parity (more than or equal to five live births) post-menopausal women have provided conflicting results. Hence, a systematic review is needed to help clarify these discrepancies and determine the effect of parity on bone mineral density in postmenopausal women.
Literature search
A multiple search strategy of electronic databases Pubmed/ MEDLINE, Google scholar and HINARI/Scirus.com were conducted in June to July, 2011 by the investigators to identify potentially relevant articles published in 1994 up until July, 2010. Searches used a combination of medical subject headings and key words (Table 1).
There were 205 hits from Pub MED/Medline, 61 from HINARI, 90 from Google scholar. All English titles and abstracts were scanned to eliminate duplicates and to assess for relevance. Additional references were found through bibliographic searches of all retrieved articles. Studies were included if they (a) examined effect of parity on BMD (by Dual energy X-ray absorptiometry or quantitative ultrasound), (b) included post menopausal women (Figure 1).
Operational definitions
Parity: Refers to the number of times a woman has given birth further definitions include:-
• Nulli parous is a woman who has never given birth
• primi parous is a woman who has given birth one time
• Bi parous is a woman who has given birth two times
• Multi parous is a woman who has given birth two or more times
• Grand multipara refers to a woman who has given birth five or more times
Bone Mineral Density (BMD): The World Health Organization (WHO) classifies BMD by T score-that is, the number of standard deviations below peak BMD-as follows: ≤1 is normal; 1 to 2.5 is osteopenia ; >2.5 is osteoporosis as measured by DEXA or a Quantitative Ultrasound (QUS).
Data extraction: The review included a study if it had clearly stated diagnostic criteria for the outcome of bone mineral density and explicitly described parity level of the study participants. Articles were classified into one of four groups according to study design (cohort, record review, case control, and comparative cross sectional) and by effect (positive, negative, no effect). Data summarized include exposure (parity) and outcome (measurement of BMD), furthermore, statistical analysis- (ANOVA, ANCOVA, Correlation and multiple regression analysis) methods, design, sample size, measurement sites, the name of the authors and the year of publication.
Quality assessment: The majority (90%) of the bone density measurement methods used in these articles includes DEXA and two studies used QUS which are considered to be gold standard diagnostics for BMD. As presented in the introduction, osteoporosis is defined by WHO as bone density that is at least 2.5 standard deviations below the mean value in a young, healthy, gender. Though a low value measured in part of the skeleton is sufficient to establish a diagnosis of osteoporosis (low BMD), over 50% of the studies used multiple diagnostic skeletal sites which increases the probability for establishing a diagnosis. The majority of the articles had adequate sample size, and over 60% of the studies were conducted in developed countries, however, there was no significant difference of the results. Though the studies included postmenopausal women, and utilized multiple regression analysis to control confounders, nearly 80% of the study designs were comparative cross-sectional studies which are considered to be low level evidence; furthermore, there was inconsistent categorization of parity throughout the reviewed articles which could be one reason for the discrepancies of the result.
| Author and year of publication | Study design | Study population | Sample size | Measurement of BMD | DEXA/QUS site | Grouping according to parity | Test statistic and Results |
|---|---|---|---|---|---|---|---|
| Hillier et al. 2003, USA [15] | Cohort | Postmenopausal women (65 or older) | 9704 | DXA and self-report questionnaire | Distal radial, spine and Total hip BMD (g/cm2) | Nulliparous, one child, two children, three children, and four Or more children | Proportional Hazards model HR= 1.44 (1.17, 1.78) Childbearing reduces hip fracture risk as a result of increased bone mass |
| Karl Michaels’ son et al. 2001, Sweden [7] | Case control | Post menopausal women (50-81) | 4640 | Questionnaire and DEXA result from record review | Proximal femur | Nulliparous, 1, 2, ≥3 | Logistic regression OR= 0.90 (0.73, 1.12), 0.75 (0.62, 0.91), 0.80 (0.66, 0.98) for Para 1, 2, and ≥3 respectively Parity and BMD associated with a reduced hip fracture risk |
| Streeten et al. 2004, Lancaster, Pennsylvania [17] | Cross sectional | Parous women aged 40 and older | 424 | DXA and self-report questionnaire | At the spine, hip, and distal Radius | 1-4, 5-7, 8-10, ≥11 | ANOVA/correlation P=0. 02 High parity is associated with increased hip BMD |
| Abourazzak et al. 2009, Moroco [21] | Cross sectional | Post menopausal women (50 and above) | 357 | DEXA and questionnaire | Lumbar spine and the total hip | Mothers with 3.7 ± 2.4 | Linear regression P= 0.01 High parity associated with higher BMD |
| Cure-Cure et al. 2002, Colombia [24] | Comparative cross sectional | Post menopausal women (50 and above) | 1855 | DEXA and questionnaire | Femoral and lumbar | Non porous and porous | Logistic regression O.R.=3.99; (1.87-8.53) The number of pregnancy increases BMD |
| Kosnayani, 2007 (MSc thesis), Ciawi, Tasikmalaya [12] | Cross sectional | Post menopausal women-44 years and above | 97 | QUS and questionnaire | Total hip | Nulli parous and parous | Multiple regression P=0. 000 A negative relationship between parity and bone density in post menopausal women |
Table 2: Increased parity reduces risk of low bone mineral density: Summary of a Systematic Review.
Study selection
Nineteen studies were reviewed; Out of nineteen studies eight of them (1 cohort, 1 case control, and four comparative cross sectional studies) concluded that parity positively influences bone mineral density (Table 2).
In contrast to the papers who reported positive effects, six studies (1 retrospective record review, 1 case control, and 6 comparative cross sectional) concluded that there is a negative effect of parity on bone mineral density in the post menopausal women (Table 3).
Five comparative cross sectional studies reported that there is no effect of parity on bone mineral density in post menopausal women (Table 4).
• Only published studies had been included, publication bias might be introduced
• Some articles were removed early for it was difficult to get the full text of the articles (Were requesting for a subscription)
• English articles were only included in the study (Resources for translation)
• The study did not consider abstracts of conference presentations, dissertations and case studies.
While genetic factors play a significant role in determining bone mass, controllable lifestyle factors such as diet and physical activity can mean the difference between a frail and strong skeleton. Amenorrhea (cessation of menstrual periods) after the onset of puberty, before menopause, and after menopause is a very serious threat to bone health and needs to be attended to by individuals and their health care providers.
This review critically examines current literature to determine the effect of parity on BMD in post menopausal women. Because the studies utilized different categorization of parity, design and methods of analysis, it was not possible to perform a formal Meta analysis of the results. However, the type of evidence, based on study type and including subject numbers, is summarized.
Of 19 studies found, six (with a combined total of 17,077 subjects) showed a positive effect of parity on BMD in postmenopausal women. Another eight studies also supported a negative effect of parity on BMD in postmenopausal women (with a combined total of 7,410 subjects). While five studies (with a combined total of 2,947 women) did not find any effect. Categorization of parity ranged from nulli-parous and parous up to grand multi-parous and analysis was made based on different classifications.
| Author and year of publication | Study design | Study population | Sample size | Measurement of BMD | DEXA/QUS site | Grouping according to parity | Test statistic and Results |
|---|---|---|---|---|---|---|---|
| Demir et al. 2008, Turkey [11] | Retrospective Record review | Post menopausal women (40-63) | 2769 | Checklist and DEXA | Lumbar spine | Nulli parous and parous | Logistic regression OR= 1.14 (1.08, 1.21) High parity was determined as a risk factor for low BMD. |
| Keramat et al. 2008, Asia (Indian and Iranian) [23] | Case control study | Post menopausal women (45 and above) | 717 | DEXA and questionnaire | Spine and femoral region | Nulliparous and >= 4 | Logistic regression OR=2. 0 (1.2-3.3) for Iran and 1.0 (1.04-1.1) in India, multi- Parity more than three are at risk of low BMD |
| Kidambi et al. 2005, Madison [27] | Comparative Cross sectional | Women ≥ 45 | 150 | Calcaneal quantitative ultrasound and questionnaire | Calcaneal bone mass | <2, >2 children | Multivariate logistic regression OR = 2.289 (1,052-4.980), p= 0.037 Women with >2 children are with low BMD |
| Jang et al., 2006, Hallym [14] | Comparative cross sectional survey | Postmenopausal women | 362 | DEXA and questionnaire | Lumbar spine | 0-2, 3-5, ≥6 | Logistic regression OR= 1.77 (0.0.57, 2.41), 2.89 (1.12, 7.42), respectively. I.e. More parity had significant negative effects on osteoporosis. Parity had significant detrimental effects |
| Maghraoui et al., 2007, Moroco [16] | Comparative Cross sectional | Postmenopausal women (40-79) | 422 | DXA and self-report questionnaire | Total hip BMD (g/cm2), and Spine T-score, | 0, 1–3 , 4–5 , and ≥6 | ANOVA/multivariate multiple regression (no of parity) P<0.0001 OR= 1.10 (1.01-1.56) Bone loss in women older than 40 is a function of parity |
| Allaliet al., 2007, Moroco [20] | Comparative Cross sectional | Post menopausal women (50 and above) | 730 | DEXA | Lumbar and total Hip | Group 1: nulliparae, group 2: 1-3, group 3: 4-5, and group 4: 6 and above | ANOVA and multiple linear regression OR=1.40 (0.70–2.80), 1.10 (0.53-2.28), 0.85 (0.39-1.80) for group 1, 2, and 3 respectively BMD of the spine and hip decreases with an increasing number of pregnancies |
| shin et al., 2010, Korea [26] | Comparative Cross sectional | Post menopausal women (40-79) | 1547 | DEXA an questionnaire | Lumbar spine and femoral neck | 3 or more children | Multivariate logistic regression OR=1. 42 (1.07,1.89) More than three offspring is at risk of low BMD |
| Lekamwasam et al., 2008, Sri Lanka [22] | Comparative cross sectional | Post menopausal women | 713 | DEXA and questionnaire | Phalangeal BMD | Group 1: nulliparous, Group 2: 1-2 Group 3: 3-4 , Group 4: more than 4 pregnancies. | Correlation and ANCOVA Group 2 and 3 high BMD, group 4 and group 1 low BMD P<0.01 Women with one to four pregnancies had the highest phalangeal BMD and BMC, while multi-parous (more than four pregnancies) and nulliparous women had lower values. |
Table 3: Increased parity increases risk of low bone mineral density: Summary of a Systematic Review.
| Author and year of publication | Study design | Study population | Sample size | Measurement of BMD | DEXA/QUS site | Grouping according to parity | Test statistic and Results |
|---|---|---|---|---|---|---|---|
| Parazzini et al. 1996. Northern Italy [19] | Comparative Cross sectional | Post menopausal Women b/n 40 and 55 | 1373 | DEXA an questionnaire | Lumbar Spine | 0, 1, 2, ≥ 3 | Logistic regression OR=0. 9 (0.4,1.8), 0.9 (0.5,1.7), 1.1 (0.5,2.2) for para 1, 2, 3 and above respectively No relationships emerged between parity and BMD |
| Henderson et al, 2000, USA [8] | Comparative -Cross sectional | Post menopausal women | 36 | DEXA and questionnaire | Lumbar spine, femoral neck and radius | Nulli parous and Grand multiparous | Non parametric (Wilcoxon test) P<0.05 No association b/n parity and BMD |
| Haddia et al, 1996, Denmark [18] | Cross sectional | Postmenopausal women of high parity | 159 | DEXA an questionnaire | Vertebrae | Average 5.1 children per women (≥5 or <5) | Correlation and regression analysis P=0. 4070 Multiparity does not influence lumbar spine bone mineral density in normal women |
| Kojima et al., 2002, Japan [25] | Comparative Cross sectional | Post menopausal women-40-69 years | 1169 | Checklist and DEXA | Lumbar spine | Nulli parous and parous | Multiple regression P=0. 643 for 40-44 years, and p= 0.358 for 60-64 years No significant correlations observed between parity and BMD |
| Lenora et al. July, 2009, Sri Lankan [13] | Cross sectional | Postmenopausal women aged (46-98) | 210 | DEXA for BMD/BMC and questionnaire | Lumbar spine or femoral neck | Nulliparous, 1–2, 3–4, and 5 or more children | ANOVA and ANCOVA P-value= 0.77, and 0.24 for lumbar spine and femoral neck (No detrimental effect on BMD among postmenopausal women) |
Table 4: No relationship between parity and low bone mineral density: Summary of a Systematic Review.
These results could be because of several changes that occur during pregnancy and lactation that can affect bone mass, including changes in reproductive hormones and in hormones that affect calcium metabolism. Since fetal and infant bone growth during pregnancy and lactation depends on calcium transfer from the mother, the possibility that pregnancy and lactation affect risk for low bone mass later in life has been investigated. Intestinal calcium absorption increases during pregnancy to meet many of the fetal calcium needs, but maternal bone losses may occur in the last months of pregnancy. The mother’s skeleton also loses bone during breastfeeding, but this loss is largely restored during weaning, as ovulation and menses are re-established. This bone loss and its subsequent restoration appear to be independent of lifestyle behaviors, including dietary calcium intake and physical activity patterns.
Clearly, a number of confounding variables influence the effect of parity on BMD, which may contribute to the divergent results in the literature.
Of 19 studies found, six (with a combined total of 17,077 subjects) showed a positive effect of parity on BMD in postmenopausal women. Another eight studies also supported a negative effect of parity on BMD in postmenopausal women (with a combined total of 7,410 subjects). While five studies (of 2,947 women) did not find any effect.
The body of evidence on parity and BMD in the literatures has several limitations including differences in the quality of the study designs, skeletal site of BMD measurement, adjustment for confounders, and demographic differences in population groups studied. Overall, the cross-sectional studies are of low quality rating. Because of the lack of evidence on the potential effects of parity on bone mineral density, the significance of the observed changes in BMD in every bone site and parity remains unclear.
Therefore, further robust, well designed observational studies should be carried out to confirm these results. Ideally, any future studies would also take into account for the consistent measurement of DEXA/ QUS sites and categorization of parities.