Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Research Article - (2018) Volume 7, Issue 4
Keywords: Ultrasound; Surface acoustic waves; Catheter; Urinary tract infection; CAUTI
Approximately 40% of nosocomial infections are urinary tract infections (UTI), and approximately 75% of nosocomial UTIs are associated with urinary catheters [1]. About 15%-25% of all hospitalized patients require catheterization [1]. Nosocomial UTIs may progress to gram negative septicemia in 30%-40% of patients. Colonization measured at more than 100,000 CFU is usually clinically associated with signs of infection requiring therapeutic intervention.
The incidence of bacteriuria in catheterized patients increases with an increase in the duration of catheterization [2]. The organisms which most commonly contaminate urinary catheters and cause the development of biofilms are biofilm-forming strains of Escherichia coli, Pseudomonas aeruginosa, Enterococcus, Proteus mirabilis and Klebsiella pneumonia [3]. These strains carry an array of adhesins in their walls, and when in contact with a surface, secrete exopolysaccharides that promote their attachment. These bacteria then multiply and spread over the surface, forming colonies embedded in a gel-like polysaccharide matrix [4,5].
The Foley catheter was originally manufactured from latex. Latex is characterized by several favorable properties, such as its capability to be processed and shaped easily, offers good resistance to gouging, has relatively high tensile strength and is low cost [6]. The drawbacks of latex include poor biocompatibility and susceptibility to encrustation and infection [7]. These drawbacks have led to the development of different types of surface coatings for the latex catheter in order to overcome these drawbacks. Coating types include biocidal coatings such as silver coating; polymeric coatings based on poly (2- hydroxyethyl methacrylate) (PHEMA), Polytetrafluoroethylene (PTFE), and silicone [8]. All of these coated catheters, depending on the specific type of coating material, offer some added advantages, such as higher biocompatibility, reduced susceptibility to bacterial colonization and to encrustation, or better lubrication [6]. However, the findings show mixed results as to the effects of surface coatings on the bacterial colonization and encrustation [6,8].
It has been shown that duration of catheterization is the most important determinant of the presence of bacteriuria [3]. The daily risk of acquisition of bacteriuria when an indwelling catheter is in situ is 3%-7%. The rate of acquisition is higher for women and older persons [4]. From 60%-80% of hospitalized patients with an indwelling catheter receive antimicrobials, usually for indications other than UTI9. This intense antimicrobial exposure means antimicrobial resistant organisms are frequently isolated from the urine of catheterized individuals [9].
Ultrasound is an acoustic wave with a frequency higher than is audible to the human ear. Bulk ultrasound is most often transmitted in the 1-3 MHz range. Low -frequency ultrasound is usually in the 100’s of kHz range. Surface Acoustic Waves (SAW) are an ultra-low frequency acoustic wave at a frequency of approximately 100 kHz. The difference between a bulk ultrasound wave and SAW is that a bulk ultrasound wave is conical, focused and penetrates approximately 10 cm. By contrast, SAW is dispersive, not focused and penetrates to a depth of approximately 3 cm.
This study evaluates the efficacy of the UroShield™ (NanoVibronix Inc., Elmsford, NY, USA) (Figures 1 and 2) for the reduction of the bacterial load in indwelling urinary catheters as well as the prevention of CAUTI. The device generates Surface Acoustic Waves (SAW) which are conducted along the length of the catheter into the bladder. The micro vibrations generated by the device prevent adhesion of the microbes on the catheter and the subsequent development of biofilm.
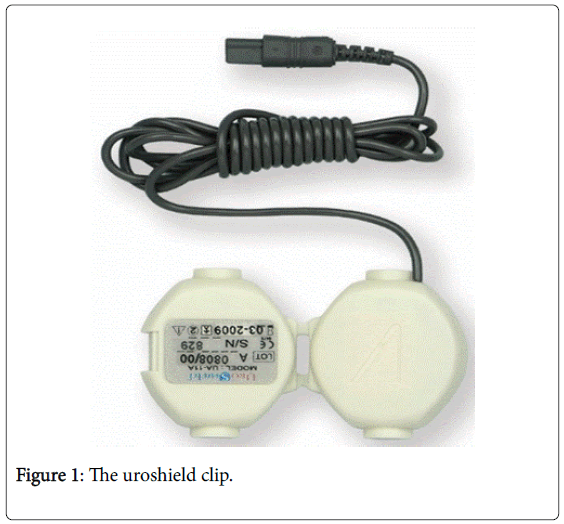
Figure 1: The uroshield clip.
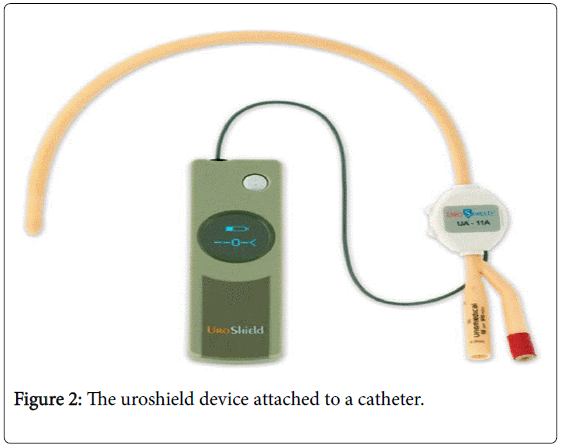
Figure 2: The uroshield device attached to a catheter.
The protocol was reviewed and approved by an IRB (Salus IRB; Austin, Tx.).
Patient selection
Fifty-five patients were selected from the residents of a network of skilled nursing facilities. All patients included in the study had an indwelling urinary or suprapubic catheter for greater than one year. All patients selected for the study had had a treated UTI in the 90 days leading up to the study enrollment.
After consenting to partake in the study, subjects were randomized to either a control group or an active treatment group. Twenty six patients were enrolled into the control group and twenty nine patients were enrolled into the treatment group.
The procedure for the two groups was identical, and both subjects and the investigators were blinded as to which group the subjects were assigned to.
Study procedure
At initiation, the current indwelling catheter was removed in a sterile technique. The distal 2 inches were cut and placed in a specimen container with 2 cc. of sterile water. A new catheter was inserted, and residual urine was collected through the new catheter into a sterile specimen container. Both the catheter and urine specimens were sent to the laboratory for evaluation.
The UroShield™ device (NanoVibronix Inc. Elmsford, NY) was applied to the catheter approximately 3 inches from the insertion in the skin (Figure 1 and Figure 2). Catheter care was performed as per the protocol of the network of Skilled Nursing Facilities. The actual devices emitted Surface Acoustic Waves (SAW) through the catheter. The sham devices behaved identically to the active devices, emitting a similar hum, but without emitting any SAW’s. The catheters and UroShield devices were left in place for 30 days until the next scheduled catheter replacement.
At the end of 30 days, when the catheter was removed, the UroShield device was disconnected, and the clip discarded. The distal 2 inches of the removed catheter was clipped and put into a sterile specimen container and 2 cc. of sterile saline was added. A new catheter was implanted, and residual urine was collected from the bladder through the new catheter, and collected in a specimen container. Both specimens were sent to the laboratory for evaluation. A new UroShield device was not reconnected.
Patients were followed for another 60 days, during which they were receiving standard catheter treatment, tracking for microbial counts in the catheters and urine, which were measured at the subsequent two scheduled catheter changes. Likewise, the number of treated infections was monitored in both groups.
Data regarding microbial counts, and infections were compared between the groups and subjected to statistical analysis.
Data analysis
Treatment effects were evaluated using between-samples t-tests, to compare the bacterial content at the end of each month with baseline levels. For each analysis, each patient’s post-treatment bacterial colonization levels were matched to their own baselines.
Improvement differences between treatment and control groups were evaluated using between-samples t-tests, to compare the change in DV levels from the baseline with each time point, between the groups. These analyses were conducted in two steps. In step 1, each patient’s DV levels at time 1, 2, and 3 were subtracted from their baseline. In step 2, the mean of the difference scores for the treatment and control groups was compared using a between samples t-test. Logistic regression was used for binary outcomes. The urinary and super urinary catheter conditions for the patients in the treatment group were compared utilizing the same analytic approach.
Colony forming units (CFUs)
At baseline the CFUs for all groups both in the catheter and urine assessment were 100K or greater. There was thus no variability between or within groups. The sham control group’s CFU counts in both the catheter and urine assessment, remained at 100K for each subsequent assessment (30, 60, and 90 days). Compared to baseline, the treatment group showed significant improvement at 30 days. There was a statistically and clinically significant reduction in the number of CFU’s in the treatment group as compared to the control group.
Mean improvement advantage in treatment vs control was 87.2K CFU), (t (53) 18.1, p<0.001) at thirty days. At 60 days the mean improvement advantage in treatment vs control was 87.5K CFU, (t (53) 18.1, p<0.001). At 90 days the mean improvement advantage in treatment vs control was 79.3K CFU, (t (53) 12.4, p<0.001).
After cessation of treatment in the active group at 30 days, there was a minimal increase in CFU count at both 60 and 90 days. In the same group, there was no statistical difference in the decrease of CFU count from 30 to 60 days after treatment, t (28)=1. p= .326, however there was a marginally significant increase in CFU from 60 to 90 days for the active group (28)=1.7 p= 0.09.
There were no differences found between the urinary and suprapubic catheters across the three post treatment months F (1,27)=0.87, p=36.
Number of treated infections
At baseline, every enrolled patient had been treated for infection during the 90 days prior to enrollment. Compared to baseline, the treatment group showed significant statistical and clinical improvement (100%) at 30 days relative to the sham control (73%). There were no reported infections in the Treatment Group while in the control group there were seven reported infections.
At 90 days after treatment, the treatment group showed a significantly stronger improvement (89.7%) compared to the sham control (46.2%). There were three reported infection in the Treatment group, while in the control group there were fourteen reported infections requiring antimicrobial therapy. (logistic regression B=2.3, Wald Chi-Square (df=1) =10.1, p=0.001.)
At 30 days post-treatment there were no treated infections for both the urinary and suprapubic catheters in the treatment group. At 90 days after treatment, the urinary catheter had fewer treated infections (4.3%) compared to the suprapubic catheter (33.3%). This difference was marginally significant B=2.4, Wald Chi-Square= (df=1) =3.2, p=0.074.
The extraordinary flexibility by which microorganisms adapt to changing environments and become shielded from environmental hazards has been at the core of the inability of chemical solutions to prevent microbial biofilm formation on implanted medical devices. Therefore, efforts to eradicate biofilms have also included mechanical methods, which, thus far, have mainly been aimed at increasing the penetration of antibiotics into the microbial colonies.[10,11]. Use of mechanical vibration energy can be used to interfere with early events in the biofilm development process, such as during the adhesion of planktonic microorganisms to surfaces, for example, [12] An additional effect of the mechanical vibration is that the chaotic microstreaming produced in fluids during the ongoing vibrations hampers the development of the concentration-dependent gradients of quorum-sensing molecules. Disruption of such gradients is likely to interfere with cell-cell communication between microorganisms, virulence factor production, and other post attachment biofilm developmental processes. In this case, the outcome could be prevention of colony differentiation and biofilm formation [13].
The device being investigated is a self-contained SAW actuator. The device is an innovative approach in which it generates low-energy elastic acoustic waves of practically nonthermal range from electrically activated piezo ceramic elements. The vibration energy is transmitted directly to indwelling medical devices in an integrated unit. The aim was to achieve dispersion of the acoustic energy on entire surfaces of indwelling medical devices with different consistencies and structures. The physical and power requirements for harnessing these waves to prevent microbial attachment and biofilm formation were analyzed. These findings were the scientific basis for the development of a product which could generate low-power acoustic waves at frequencies ranging from 100 to 300 kHz.
The use of the term treated UTI in this study is defined as any elevation of microbial count, combined with symptoms causing the treating physician to initiate antimicrobial therapy.
This study was designed to evaluate both the efficacy of the UroShield device on decreasing microbial counts on indwelling catheters and in the bladder, as well as evaluate the device’s efficacy in preventing treated infections.
The UroShield device was extremely effective as a bactericidal agent. The device was able to reduce the CFU count from 100,000 to 10,000 CFU or less in 25 of the 29 patients within the treatment group (p value of <0.001 compared to control). Importantly, this resulted in a highly statistically significant decrease in the incidence of symptomatic UTI.
Almost immediately after insertion of a urinary catheter, bacterial colonization occurs. As the colonization increases, it approaches a critical mass where the area is termed infected. When this numerical (or non-treated) infection begins to produce symptoms, the treating physician will decide on the initiation of utilizing antimicrobials therapy. There is low efficacy related for antibiotics in preventing CAUTI [14]. Antibiotics have also been shown to poorly prevent biofilm formation in catheters, which may begin to occur within a few hours of placement [15,16].
The formation of biofilm entails several simultaneous physiological phenomena, including adherence of the microorganisms either to a surface or to one another, subsequent alteration of gene expression, and formation of an extracellular matrix, most often polysaccharide based [17]. It is specifically to these properties that the investigated device is targeted. SAW is an acoustic wave that resonates in the 90-100 kHz range. These short acoustic waves create a micro vibration affect, barely felt by the nociceptors on the skin. This micro resonant effect creates an inhospitable environment for the initial microbes to adhere to the catheter surface.
Acoustic waves travel well in a hydrated medium, which is the property that helps to conduct the SAW along the length of the catheter, and into the bladder. The acoustic waves generated by SAW is also believed to alter the quorum sensing of the microbes. This alteration of the signaling between cells also helps to delay and disrupt the formation of the biofilm and its extracellular matrix. It is believed that the hostile environment, together with the ongoing acoustic assault of the SAW on the microbes, generates the bactericidal effects of the investigated device (Figure 3).
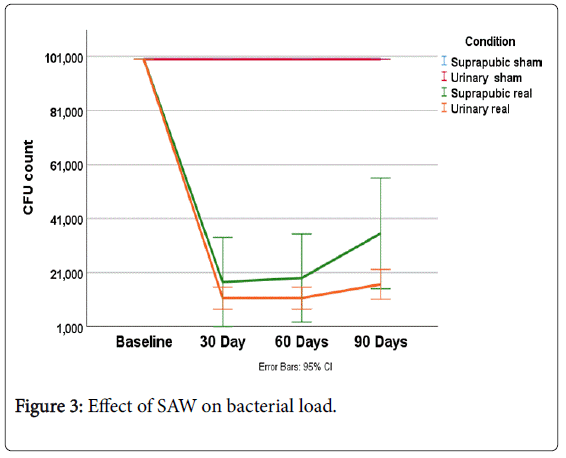
Figure 3: Effect of SAW on bacterial load.
This study was a double blinded, randomized controlled trial. This study design removed the bias of different patients being treated differently by the medical personnel. In addition, because the study was conducted in a single network of Skilled Nursing Facilities, with a unified treatment protocol, the catheter care provided was similar, eliminating built-in bias because of differential treatment at different facilities.
The catheters used in this study were an all Silicone, uncoated model, so that the presence of an antimicrobial agent would not be a confounding factor.
The results showed that during the course of treatment, certain species of bacteria were eradicated. There was no predilection for any specific species. In different subjects, different species were reduced or annihilated.
The species that survived began to multiply in the follow-up period, after removal of the device. However, the rate of reproduction and multiplication was significantly slower than was observed in the control group. These results are consistent with the understanding that treatment with the UroShield device has a bactericidal effect, and also alters the remaining living microbes to such an extent that their viability is significantly altered (Table 1).
| Proteus mirabilis |
| E. coli |
| Providencia rettgeri |
| Candida albicans |
| Pseudomonas aeruginosa |
| Klebsiella pneumoniae |
| Serratia marcescens |
| Morganella morganii |
| Alcaligenes faecalis |
| Staphylococcus aureus |
| Citrobacter freundii |
| Acinetobacter baumanii |
| Providencia stuartii |
| Klebsiella ornithinolytica |
| Enterococcus faecalis (Group D) |
| Aerococcus urinae |
Table 1: Species cultured from the subjects.
The CFU count of bacteria in this study was significantly lower in the study group compared with the control group, both in the evaluation of the distal tip of the catheter, as well as the retained urine in the bladder. Because the urinary catheters were left in place for 30 days, except in emergency conditions, as per the facility protocols, there was no difference in catheter placement length between the treatment and the control groups. The removal of this confounding factor is important as the length of time the catheter is in place is directly correlated to the degree of colonization and biofilm formation [14].
The limitation of this study is that it only evaluated the distal tip of the catheter as well as the retained urine, as opposed to evaluating the catheter in its entirety. Because microbes can adhere to encrustation which can occur within the first hour of catheter placement, it is possible that some biofilm formation might have begun at the proximal end of the catheter. The clinical results of the study, as well as the fact that the SAW source, meaning the strongest acoustic wave, is generated near the proximal portion of the catheter, contradict this assumption, but it is a subject that should be evaluated.
This study evaluated both the immediate and longer-term effects of the investigative device. By evaluating the results during the active treatment period, and then extending the evaluation 60 days post treatment, assessments were able to be made on the long-term effects of the device-during the critical colonization stage, during the development of biofilm and in the prevention of infections.
The UroShield™ device was shown to be effective in significantly reducing the number of CFU’s in patients with indwelling catheters. It was also shown to be effective in reducing the number of treated UTI’s in this patient population. SAW in the form of the UroShield™ device is an effective tool in the prevention of CAUTI and while further evaluation is encouraged, can be safely utilized with a high likelihood of success.