Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Review Article - (2016) Volume 4, Issue 2
The concept of assisted reproductive technologies was most notably derived from the late 19th Century experiments of Sir Walter Heape who successfully transplanted rabbit embryos. Interestingly, it was not until the late 1940’s and 1950’s that renewed interests in rabbit embryo transfer and cryobiology occurred. The history behind developing effective procedures can be fascinating, though few could be more accidental than Dr. Chris Polge’s discovery of glycerol (1948), from a mislabeled bottle of sugar solutions, being an effective cryoprotective agent for sperm freezing. The purpose of this review paper is to discuss four key scientific breakthrough technologies occurring between 1985 and 1995, which ultimately shaped the future of today’s human in vitro fertilization (IVF) industry. More importantly, this paper highlights the foundation of underlying related discoveries and some unique stories involving their development and publication. In the end, this paper emphasizes the value of understanding scientific discovery timetables and the eventual re-discovery in the hands and minds of creative, determined and dedicated scientists, as history tends to repeat itself before its useful application is realized.
<Keywords: ICSI, PGS, Laser zona dissecton, Vitrification, Assisted reproductive technologies
The applications of today’s assisted reproductive technologies in human infertility have seemingly evolved in a fairly predictable manner, or have they? Typically beginning with historic and often intriguing animal modeling efforts, there is generally an initial purpose that ends up with more diverse implications when used in Reproductive Medicine. At times the technical incorporation and acceptance by scientists is slow and progressive, before its importance is ultimately widely accepted. Case in point is both the evolution of preimplantation genetic screening of embryos and the recent conversion to vitrification for their cryopreservation. Whereas, other important technologies like sperm injection and laser ablation have had an immediate impact with worldwide acceptance. But what was the origin of these breakthroughs in technology, and their associated stories? The purpose of this communication is to contrast the historical evolution of these four critically important assisted reproductive technology procedures, which have been successfully integrated to establish an irreplaceable foundation in the success of today’s IVF industry.
Early efforts to sex rabbit embryos [1] were initiated by two brilliant pioneers in Reproductive Biology, both of whom were knighted by the Queen of England, Drs. Richard Gardner and Robert Edwards. The eloquent, fascinating and in-depth history behind Dr. Edwards interests in cytogenetics, prior to IVF, has been reviewed in his life’s story [2]. The story also alludes to a formidable team of young scientists emerging in the UK in the 1960’s and 1970’s (in association with Cambridge University, Oxford University, the Marshall Laboratory and the Medical Research Council) who shaped the future of Reproductive Genetics, Immunology and Physiology, as we know it today. Many of the latter scientists (e.g., R Yanagamachi, MH Johnson, A Handyside, R Gosden, J Rossant, G Papaioannou, A Surani, D Whittingham, A Trounson, S Willadsen and others) made pioneering discoveries and contributions to the fields of Embryology, Genetics and Reproductive Medicine, which will not be discussed in this review. By the 1980’s, an alternative to karyotyping was identified by detecting the histocompatibility antigen of the Y chromosome of murine embryos (H-Y antigen) [3,4] and applied to embryo sexing in animal agriculture [5-7]. It is noteworthy to mention that Dr. Ken White’s doctoral research was presented at the 1982 International Embryo Transfer Society meeting and was the recipient of the first inaugural Student research award [8]. Ultimately, the emphasis on genetic determination led to the development of preimplantation diagnosis (PGD) in the mouse model [9,10]. In conjunction with the specific polymerase chain reaction (PCR) testing for X and Y chromosomes [11-13], simultaneous efforts to improve the efficacy of single cell biopsying [14] facilitated human PGD development [15,16]. In reviewing the history of PGD between 1990-2010, Handyside [17] eludes to early errors in sex determination by PCR, prior to nested PCR, and the importance of utilizing multicolored fluorescence in situ hybridization (FISH) to more reliably identify X and Y chromosomes. The technology of “chromosome painting” was adapted to embryos by Santiago Munne et al. [18], and extended to include up to 12 different probes and sequential analyses of fixed nuclei to facilitate preimplantation genetic screening (PGS) for aneuploidy determination [19]. Improvements in euploidy and translocation diagnostic capabilities progressed from FISH to array comparative genomic hybridization (aCGH), allowing 24 chromosome types to be clinically evaluated [20,21]. In turn, aCGH reduced the error rate and diagnostic limitations of FISH resulting in lower spontaneous abortions and fewer implantation failures [22]. Next generation sequencing (NGS) [23-26] has further enhanced the speed and precision of aneuploidy testing, through massive parallel genome sequencing [27,28]. The history of PGS/PGD technologies in assisted reproductive technologies is still being created as dynamic growth is ongoing. Meanwhile, the full impact of today’s PGS capabilities would be impossible without the advent of vitrification as a highly efficient cryopreservation procedure. Together, the transfer of vitrified-warmed single human euploid blastocysts is capable of achieving >70% implantation rates, independent of age [29].
Behind the cryobiological principle and potential advantages of freezing without potentially damaging ice formation (i.e., forming a metastable glass state), neither Drs. Greg Fahy nor William F. Rall could have foreseen the tremendous effectiveness that vitrification would have on maintaining the cryo-viability of oocytes and embryos. Dr. Fahy’s dreams were, and still are, fixated on the much bigger challenge of whole tissue/organ preservation [30,31]. All the while, Dr. Rall wanted to simplify conventional embryo cryopreservation procedures for onfarm use, and possible in-field conservation efforts, without a need for electronic equipment [32]. However, it was an extremely competitive time among scientists, as new breakthrough technologies were rapidly developing. Bill Rall conducted a series of clandestine experiments in a walk-in cold room at the American Red Cross Blood Research Lab (Bethesda, MD) [33]. These experiments were secretively performed with the support of the Scientific Director, Dr. Harold Merryman, knowing that fellow scientist, Dr. Tsuneo Takahashi, was conducting vitrification studies on monocytes [34]. Knowing this, Bill Rall strived to publish their mouse embryo vitrification success in Nature as soon as possible [35], meanwhile he intentionally delayed a manuscript review of the unknowing Dr. Takahashi. Dr. Merryman later regretted the support he extended Dr. Rall to keep his project secretive, as evidenced by offering his famed scientific memoirs to Dr. Takahashi upon his death. The third generation of Dr. Rall’s vitrification solutions (VS3a, a 6.5M glycerol solution) was proven safe for use under ambient conditions, achieving comparable survival levels and pregnancy outcomes to conventional slow freezing of mouse (with trustworthy collaborators in England) [36] and sheep blastocysts (mentoring a local PhD candidate) [37,38]. Ironically, Dr. Rall delayed the latter published paper in the sheep for 3 years, hoping to publish the first vitrified large mammal birth in the cow (unpublished data, conducted with Dr. Stanley Leibo.)
Although alternative low toxicity vitrification solutions were first reported in 1990 [39], nearly a decade passed before being proposed for improved assisted reproductive technologies application on human oocytes, cleaved-embryos and blastocysts [40,41]. This interest in clinical vitrification was linked to the formation of unique cryo devices like the open pulled straw [42,43], cryoloops [44-46] and cryotops [47,48], whose thin surrounding film of vitrification solution and direct contact with LN2 achieved ultrarapid cooling rates. Furthermore, our understanding of vitrification solutions and their potential toxicity were enhanced by Drs. Jill Shaw [49,50], Jaffar Ali [51], Miyake Kasai [52] and Tetsunori Mukaida [53] and their co-workers. By the mid-2000’s, it was the commercial industry, developing new devices and solutions that propelled vitrification use into IVF labs, for better or worse. By 2010, the benefits of vitrified embryos and oocytes having virtually no change from their fresh state was gaining worldwide acceptance. During this time, the relative importance of warming rates to insuring successful vitrification [54] was proven in a murine experimental model system by Drs. Seko Seki and Peter Mazur (“the father of modern cryobiology”). These findings supported the effective development and use of aseptic, closed vitrification device systems [55-60], proving that open device systems were not a requirement for successful outcomes. Yet, the relative importance behind the myth of open devices and their ability to achieve ultra-rapid cooling rates continues to-date. It is important to realize that these highly effective devices require equally rapid warming rates, if not more, to optimize survival [61-64]. Thus, open system devices are more susceptible to technical variation and user error associated with device handling, as well as lacking the secure storage capacity of a closed system. In short, a key component to optimizing post-warming survival, independent of device used, is to insure the warming rate is greater than the cooling rate; of which the need for speed is inversely correlated to the concentration of the cryoprotective agent used [62,64]. Although it took more than 20 years of development, vitrification has transformed the IVF industry, with regards to oocyte cryobanking [65,66] and the justified adoption of vitrification-all IVF cycles [67]. As the story continues to unfold, in terms of devices and vitrification solutions, today blastocysts are vitrified with great confidence that their fresh-state viability will be completely sustained. This is particularly true in conjunction with blastocyst biopsy/PGS-single embryo transfer applications [68,69] where over 99% survival can be typically achieved [29].
Sustaining the complete cryosurvival of blastocysts was dramatically improved by blastocoele collapasing tatics for cryopreserved embryos. As with assisted hatching procedures in the 21st Century, blastocyst collapsing was easily and safely achieved using a non-contact, infrared (IR) laser device [70]. The incorporation of laser zona and cellular ablation has also greatly simplified and improved the efficiency of trophectoderm biopsying procedures [71,72]. But how did laser technology get implemented into Reproductive Medicine? Following early gynecological surgery applications [73], lasers were thrust into the biomedical field in the mid 1980’s, in conjunction with a surge of US-federal funding for “Star Wars” research. One example of the early advanced technology was the development of the Meridian fluorescence microscopic workstation with its computer automated programmable stage and built-in Excimer ultra-violet (UV) laser, allowing for the preselection of cells to ablate (Figure 1). Laser beams were effectively used to selectively destroy cells [74], dissect the zona pellucida [75,76] and even created force fields capable of moving chromosomes [77] and sperm [78]. However, most of these early efforts proved impractical and/or incorporated the use of strong UV wavelengths [74,76], which were potentially damaging to the genetic integrity of cells. Feichtinger exhibited the effectiveness and safety of a longer wavelength laser (2100 nm; [75,79]), however it required an optical fiber-touch procedure which did not simplify matters in contrast to assisted hatching using a micropipette and acidic Tyrode’s solution [80-83].
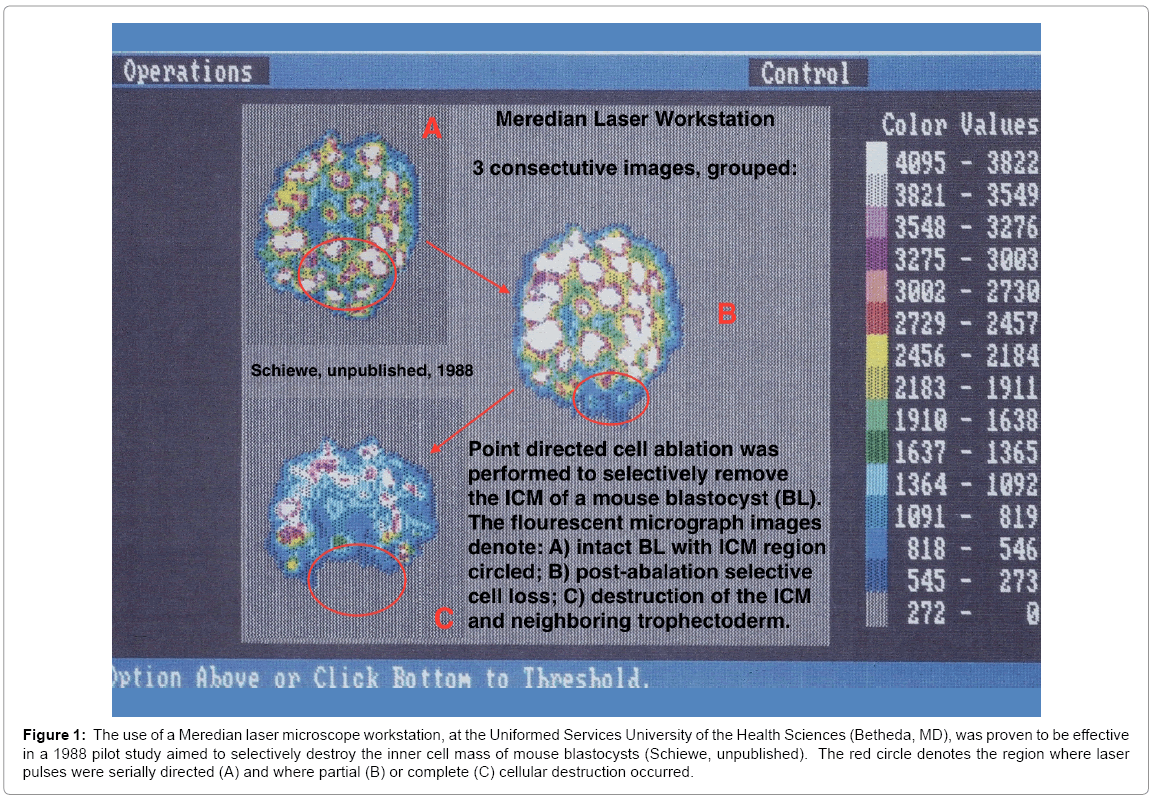
Figure 1: The use of a Meredian laser microscope workstation, at the Uniformed Services University of the Health Sciences (Betheda, MD), was proven to be effective in a 1988 pilot study aimed to selectively destroy the inner cell mass of mouse blastocysts (Schiewe, unpublished). The red circle denotes the region where laser pulses were serially directed (A) and where partial (B) or complete (C) cellular destruction occurred.
It was the simultaneous development of non-contact IR laser systems in the mid-1990’s in Europe (1084 nm: [84,85]) and the USA (2100 nm: [86,87]) that allowed the technology to progress safely into the assisted reproductive technologies field. The holmium:yttrium scandium gallium garnet (Ho:YSGG) laser system devised by Dr. Yossi Neev was effective (Figure 2) but involved a large box device requiring extensive mirror calibrations. Meanwhile, the compact nature and simplicity of the diode laser (1084 nm) developed by Swiss researchers, made the Ho:YSGG efforts practically obsolete upon publication. Cell Robotics (Albuquerque, NM) initially integrated the diode laser into a microscope workstation, and conducted FDA trials in the late 1990’s. Although no more effective than assisted hatching with acidic Tyrode’s solution, it was apparent that its greatest impact would be aiding embryo biopsy procedures [88,89]. Both the simplicity and efficacy was improved by eliminating the need for a dual microtool micromanipulation approach. The technology was acquired by Hamiliton-Throne (USA) and Research Instruments (Europe), whom developed the incredibly useful computerized devices used today, in conjunction with daily embryo evaluations and micromanipulation procedures with the simple “energized” touch of a bottom.
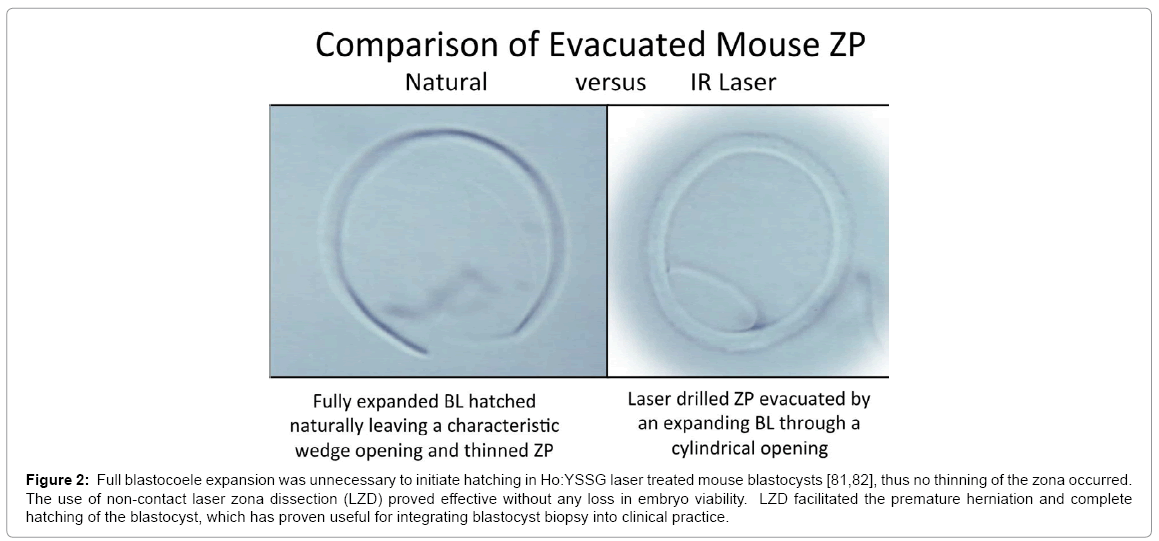
Figure 2: Full blastocoele expansion was unnecessary to initiate hatching in Ho:YSSG laser treated mouse blastocysts [81,82], thus no thinning of the zona occurred. The use of non-contact laser zona dissection (LZD) proved effective without any loss in embryo viability. LZD facilitated the premature herniation and complete hatching of the blastocyst, which has proven useful for integrating blastocyst biopsy into clinical practice.
Today, in addition to routine assisted hatching and selective cell ablation applications, zona dissection may be used to assist intracytoplasmic sperm injection (ICSI) efforts [90], potentially reducing oocyte trauma associated with attempted penetration of a non-compliant hardened zona pellucida or caused by using dull, poor quality injection pipettes. More recently, an IR laser has been used to significantly elevate the warming rate of a vitrified sample (107 °C/min; [91]), an application which is much more likely to have an important applied impact. Overall, the ease of laser use has greatly simplified and improved the efficacy of many assisted reproductive technology procedures.
Inarguably, the most revolutionizing assisted reproductive technologies procedure used in Human IVF was the development of ICSI. Most individuals are familiar with the breakthrough efforts of an Italian Physician, Dr. Gianpiero Palermo, experimenting with sperm injection at the Universitair Ziekenhuis fertility clinic in Brussels, Belgium, where the first human birth was reported in 1992 [92,93]. Like other scientists of his day, he initiated his Reproductive career in male infertility studies with sub-zonal insemination [94] in the mouse model [95] as well as working with discarded immature human oocytes. In late 1991, the latter preliminary investigations yielded unexpected outcomes. Applying an unconventional direct 3 o’clock sub-zonal insemination injection approach, not surprisingly (i.e., in hindsight) Dr. Palermo punctured directly into the egg at times, injecting a single sperm into the egg cytoplasm and not the perivitelline space. The efficacy of the resulting subsequent pronuclear formations was often better than the sub-zonal insemination outcomes, which gave him the foresight and courage to shift his procedural emphasis.
The rest was history [92], unlike the earlier efforts by Lanzendrof and coworkers at the Jones Institute in Norfolk, VA [96], whom performed a preclinical sperm injection study with notable fertilization, but their corresponding unsatisfactory cleavage development, tainted their perspective, as they chose to not implement ICSI clinically. Those efforts followed the successful use of sperm injection in the rabbit model [97]. Indeed, it was these Japanese investigators who pioneered the useful application of sperm injection more than a decade after the injection of a human sperm into a hamster oocyte was proven capable of experiencing decondensation of the sperm head (i.e., pronuclear formation; [98]). Where progress with ICSI really stumbled, was in the early failed efforts by Clem Markert [99] using a murine model system. Years of efforts and a dismal lack of in vitro success, led to a discontinuation of his and others experimental efforts. Ironically, it was later proven by Huang, Kimura and Yanagimachi [100] that ICSI using mouse oocytes simply required the mechanical assistance of a piezo-injector system to efficiently and routinely achieve high fertilization rates.
By that point, the application of ICSI in human IVF had attained worldwide acceptance for the treatment of male factor infertility, based predominantly on the concerted efforts by a dedicated team of Embryologists under the direction of Dr. Andre Van Steirteghem (Joris, Liu, Nagy, Crabbé, Verheyen and others). The mystic to their success was unheralded, as international visitors repeatedly attended ICSI Workshops conducted by the Brussels group (between 1993-95). It is worth mentioning that another European scientist experimenting with sub-zonal insemination post-1990, Dr. Michael Tucker, was also dabbling with the concept of direct egg injection (DEI) based on Susan Lanzendrof ’s early work. Fertilization success was achieved, although its efficacy at that time was no better than sub-zonal insemination, especially when they factored in elevated degeneration rates (associated with the use of 10 μm OD injection pipettes) and difficulties in isolating/ injecting single sperm in the absence of PVP use. Although his early success with DEI at the Reproductive Biology Associates in Atlanta, Georgia involved mixed transfers and was unpublished, it is humorous to note that in some presentations Dr. Tucker hybridized the name of his procedure with ICSI (i.e., never a big fan of the acronym) to jokingly coin the acronym “DICSI”, for his association with southern American living [101]. On another occassion, Dr. Tucker attempted to publish the term Sperm Head Injection Technique (i.e., SHIT) which aroused a good laugh by the editor of Human Reproduction, Dr. Bob Edwards, but it never made it into press [102]. “ICSI” it was, as still other early clinical efforts independently proved their injection procedures were efficacious for severe male factor sperm [103,104], and that alternative microinjection approaches and microtool-manufacturing equipment could be effectively used [101,105].
In conjunction with early oocyte cryopreservation efforts, ICSI proved to be vital to achieve reliable post-thaw fertilization rates [106,107]. In the Gook et al. [106] study, embryo transfers were not attempted but it is noteworthy that 43% of the ICSI-derived zygotes formed blastocysts, following slow freezing in 1.5 M propanediol. Based on Dr. Debra Gook’s success, the evolution of oocyte freezing was rekindled with live births reported in the USA [108], and in Italy [109] where she had scientifically consulted in 1996. By the end of the 20th Century, nearly every IVF Lab in the world possessed the capacity to perform ICSI and resolve most male factor infertility issues. Despite fears associated with epigenetic factors and potential genetic anomalies, today ICSI use is widespread. In fact, because of its high reliability and rare, unexplained cycle fertilization failures, many programs have routinely adopted it as the preferred fertilization method, replacing conventional IVF.
The decade between 1985 to 1995 marked the most productive and creative period of technological advancement in mammalian embryology, as it pertains to todays’ human IVF industry. The development of ICSI, laser manipulations, vitrification and preimplantation genetic testing established a solid foundation for the efficient and effective treatment of human infertility. The stories told reveal some unique insights into historic developments which took decades to be fully appreciated. Like much of science, there seems to always be another layer of detail to be learned. The same is true with historical events in science. For example, there was decades of scientific discovery and development in invertebrate species and other living cells, concurrent or prior to the mammalian models discussed above. What they all had in common was the creative vision, determination and dedicated efforts of scientists with a passion to ask questions, take chances and learn through experimentation.
This paper is dedicated, in part, to the memory of Dr. Peter Mazur, who taught cryobiology to all of us, directly and through his fellows. Furthermore, he contributed to our understanding of vitrification and the importance of warming events up until his final day (December 30, 2015). I had the good fortune to have had a few insightful communications/conversations with Dr. Mazur in the last year, and for that I am truly grateful. Overall, this paper is a tribute to the pioneers, creative thinkers and those who persevered with historical ideas to help make them a practical reality in Human assisted reproductive technologies. In the words of my first Reproductive Physiology mentor, Dr. Perry Cupps in 1976, “it is important to study the history of Reproductive Physiology and its technological advancement, as history tends to repeat itself, gaining new momentum in subsequent decades”. I believe the historical stories told herein, about four historical assisted reproductive technology procedures of importance today, support Dr. Cupps’ theory. In addition, I would like to thank and graciously commend the honesty and willingness of several colleagues who revealed their stories, some never disclosed publicly before, in an attempt to tell the real truth behind some historical events. These individuals included Drs. Greg Fahy, Gianpiero Palermo, Michael Tucker, Ken White and Santiago Munne.