Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2012) Volume 1, Issue 4
Aim: The aim of this study was to investigate whether Harmonic Scalpel (HS) increases the complication rate in the patients undergoing neck dissection in patients with Papillary Thyroid Carcinoma (PTC).
Methods: 95 patients with PTC undergoing bilateral total thyroidectomy and central or lateral neck dissection were included in to study. Patients whom heamostasis was carried out using HS at each stage of the operation were classified as group I (n=52), and patients whom heamostasis was performed without HS in the dissection of nerves and in the dissection of regions containing parathyroids and ductus thoracicus as Group II (n=43). Groups were compared in terms of operation time, postoperative nerve injury, hypoparathyroidsm and development of chylous fistula.
Results: Demographic data, stage of tumor and type of operation were similar between groups. Mean operation time was 19 min. shorter in group I (p=0.003). There was no difference in nerve injury and hypoparathyroidsm between groups. Chylous fistula was seen in 3(5.7%) patients in group I. It was not seen in group II.
Conclusion: Use of HS in patients with PTC undergoing neck dissection decreases operation time significantly without increasing the rate of nerve and parathyroid injury, but may increase the risk of development of chylous fistula.
<Keywords: Harmonic scalpel; Neck dissection; Papillary thyroid carcinoma
Surgical principles established by the pioneers of thyroid, were good exposure of thyroid gland, clear identification of nerves, parathyroid glands and perfect heamostasis [1]. New vessel sealing technologies Ligasure (Covidien, Boulder, Colorado) and Harmonic Scalpel (Ethicon Endo-Surgery Inc, Cincinnati, Ohio) have emerged in the recent literature [2-4].
Harmonic Scalpel (HS) is a new promising tool introduced to surgery two decades ago. It uses high frequency (55,500 Hz) mechanical energy to cut and coagulate tissues at the same time. Mechanism of HS depends on denaturation of protein by using ultrasonic vibration to transfer mechanical energy sufficient to break tertiary hyrogen bonds [5,6]. Proposed advantages with its use include less thermal tissue damage to adjacent structures as compared with electrocautery and reduction in the operative time due to combination of simultaneous cutting and coagulation functions [7].
There have been several recent studies investigating the safety of HS in patients undergoing thyroidectomy [8-10]. Most studies conclude that use of HS decreases both operative time and intraoperative blood loss and provides benefits in postoperative pain without increasing complication rates when compared to conventional techniques [7-11].
The aim of this prospective randomized study is to evaluate the effect of HS on complications in dissection of left lower neck region and parathyroid glands and nerves (recurrent inferior laryngeal nerve, vagus, accessory, phrenic and hypoglossal) in patients with papillary thyroid carcinoma (PTC) undergoing central or lateral neck dissection.
After approval was obtained fom local ethical committee, informed consent was taken from 104 patients undergoing operation for stage II-IVa PTC. Of these, 6 patients using warfarin. 1 patient who has RILN injury due to a previous operation and 2 patients with hypoparathyroidism were excluded from the study (Figure 1).
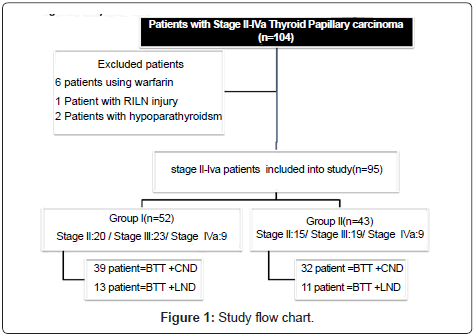
Figure 1: Study flow chart.
Of 95 patients included in the study, 71 underwent bilateral total thyroidectomy (BTT) and central neck dissection (CND) and 24 underwent BTT and lateral functional neck dissection (LND). All operations were performed by the same surgical team. The surgeon was blinded to the technique to which the patients were assigned upon opening the envelopes in the operating room, just before surgery. Patients in whom heamostasis was carried out using HS at each stage of the operation were classified as group I (n=52), and patients in whom heamostasis was performed without HS in the dissection of nerves (recurrent laryngeal nerve, vagus, accessory, phrenic and hypoglossal nerve) and in the dissection of regions containing parathyroids and ductus thoracicus as Group II. (n=43). In regions where HS was not used, standard tying and hemoclips were used.
Surgical Technique
Patients whose preoperative and intraoperative findings indicating stage-I PTC underwent only BTT and were excluded from the study. Patients who were at Stage II-IVa were included into the study. Patients with stage II-III PTC and patients with stage III(T3N1a)-IVa underwent BTT and CND, BTT and LND respectively. Extracapsular resection was used for total thyroidectomy in a standard manner, which included the following steps. Under general anesthesia, the patients were placed on the operating table in the supine position with the neck extended. A standard incision was made 2-3 cm above the sternal notch. Subplatysmal skin flaps were made. The strap muscles were divided in the midline and retracted laterally. Thyroid was retracted medially and middle thyroid vein was sealed with HS. The recurrent laryngeal nerves were identified and preserved bilaterally in all patients. The superior pole of the gland was dissected gently to avoid injuring the superior laryngeal nerves. The superior and inferior thyroid arteries and veins were controlled using HS. The parathyroid glands were identified carefully, vascular pedicle of them were preserved. Parathyroid autotransplantation was carried out as needed. Parathyroid glands used in autotransplantation were checked by frozen section before the procedure. After total thyroidectomy was completed, lymph nodes especially placed in lateral compartment were examined with frozen section for metastasis and then CND followed. Anatomically, the central compartment (level VI) is surrounded by, the hyoid bone superiorly, and the thoracic inlet inferiorly and the carotid sheaths laterally. A CND involves removal of all level VI lymph nodes, which include the pretracheal and paratracheal, precricoid (Delphian), and perithyroidal lymph nodes, and those along the recurrent laryngeal nerves. After CND, head of the patient was rotated to contralateral side and apron incision was made. The LND (modified radical neck dissection) involved removal of all soft tissue and lymph nodes in levels IIa to V. The sternocleidomastoid muscle, jugular vein, carotid artery, vagus nerve, phrenic nerve, and spinal accessory nerve were preserved.
In the dissection of left lower part of neck, especially in the medial of internal jugular vein, ductus (Figure 2) thoracicus was tried to be seen. In the dissection of this region, heamostasis was performed by HS in Group I and by nonabsorbable suture in group II. In the dissection of nerves (RILN, vagus, accessory and phrenic nerves) and of paratyhroids, heamostasis was performed by HS in Group I and by standard tying and hemoclips in Group II. Closed suction drain was placed in all patients at the end of the operation. The wound was closed using 3-0 polyglactin (Vicryl; ETHICON) for the muscular fascia and subcuticular 4-0 poliglecaprone (Monocryl; ETHICON) for the skin.
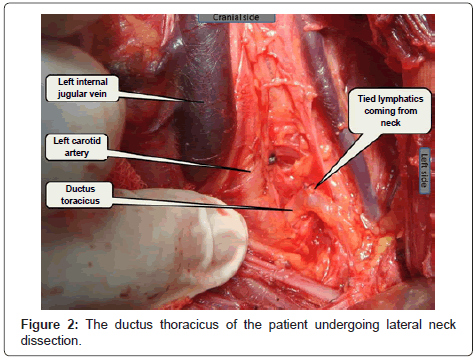
Figure 2: The ductus thoracicus of the patient undergoing lateral neck dissection.
Demographic data of the patients, (Table 1) their stages, the type of dissection, the number of removed and metastatic lymph nodes, duration of operation, duration of hospitalization, and postoperative complications were recorded (Table 2). All patients were questioned on postoperative first day for hypocalcemia symptoms and signs. Those with a calcium level below 8 were considered to have hypocalcemia and administered oral calcium and vitamin D. Patients whose hypocalcemia lasted for more than 6 months were considered permanently hypocalcemic (Table 3). All patients were seen for follow-up at 2 weeks, 1 month, and 6 months after operation. Specialists from the hospital’s otolaryngology department, blinded to the treatment groups, performed a direct laryngoscopy before operation and 2 weeks after operation in all patients. In the presence of abnormal movement or position of right or left vocal cord, follow-up nasopharingolaryngoscopy studies were performed at 6 month after operation.
| Group I (n=52) | Group II(n=43) | p | |
|---|---|---|---|
| Female/Male | 45/7 | 34/9 | 0.333 |
| Age±SD | 55.3±10.2 | 52.3±5.7 | 0.089 |
| BMI±SD | 27.5 ±5.2 | 28.6±6.3 | 0.353 |
Table 1: Demographic data of the patients.
| Group I | Group II | p | |
|---|---|---|---|
| Mean duration of Operationi±SD | 117.6±30.5 | 138.8±37.9 | 0.003 |
| Mean duration of hospitalization ±SD | 3.4± 4.7 | 2.4 ± 1.3 | 0.180 |
| The distribution of PTC patients according to stage II/III/IVa | 20/23/9 | 15/19/ 9 | 0.885 |
| The number of patients undergoing BTT + CND (%) | 39(75%) | 32(74.5%) | 0.948 |
| The number of dissected LAP in patients undergoing CND ±SD// Percentage of patients with metastatic Lap. //The number of metastatic lap ±SD |
10.4±3.4 / 22(56.4%) 1.3±1.09 |
11±2.5 / 19(59%) 1.15±1.17 | 0.409 0.801 0.578 |
| The number of patients undergoing FLND (%) | 13(25%) | 11(25.6%) | 0.948 |
| The number of dissected LAP in patients undergoing FLND ±SD // The number of metastatic LAP ±SD |
28.8±8.9 / 5.9± 3.9 | 31.4±7.3 / 6.8±3.8 | 0.448 0.574 |
| The number of patients in whom ductus thoracicus was seen | 4(7.7%) | 5(11.6%) | 0.727 |
Table 2: Stage of PTC, type of disection , duration of operation, and hospitalization.
| Group I(n=52) | Group II(n=43) | p-value | |
|---|---|---|---|
| The number of chylous fistula (%) | 3(5.7 %) | 0 | 0.249 |
| The number of patients with transient hypocalcemia (%) | 7 (13.5 %) | 6 (14.0%) | 0.945 |
| The number of patients with permanent hypocalcemia (%) | 2(3.8 %) | 1(2.3%) | 1.000 |
| Transient RILS injury (%) | 1(1.9%) | 2(4.6%) | 0.588 |
| Permanent RILS injury (%) | 0 | 0 | - |
Table 3: Postoperative complications.
Postoperative chylous fistula development was evaluated. In patients with chylous fistula, the day when fistula was noticed, daily flow output, treatment methods and duration of chylous fistula were recorded. Oral nutrition was discontinued in these patients and total parenteral nutrition commenced. Sandostatin treatment was initiated. The heads of their beds were lifted and compressive bandaging and daily wound care was carried out.
Statistical Analysis
Data analysis was performed by using Statistical Package for Social Sciences (SPSS) version 11.5 software (SPSS Inc., Chicago, IL, United States). While, the continuous variables were expressed as mean ± SD, otherwise, number of cases and (%) were used for categorical data. The mean differences between groups were compared by Student’s t test. Categorical data were analyzed by Pearson’s Chi-square or Fisher’s exact test, where applicable. A p value less than 0.05 was considered statistically significant.
There was no difference between two groups in terms of demographic data (Table 1). Both groups were homogenous with regard to tumor stage. 39(75%) patients in Group-I underwent CND, and 13(25%) LND. In Group-II, 32(74.5%) patients underwent CND and 11(25.6%) LND. There was no difference between groups in terms of dissected and metastatic lymph nodes (Table 2).
In Group I, transient hypocalcemia developed in 7(13.5%) patients and permanent hypocalcemia in 2(3.8%) patients while in group II they developed respectively in 6(14%) and 1(2.3%) patients (table 3). Transient RILS injury occurred in 1(1.9%) patient in group I, in 2(4.6%) patients in Group II (p=0.94). Permanent RILS injury, bleeding, esophagus and trachea fistula occurred in neither group. Mean duration of operation was significantly shorter in Group I than in Group II (table 1) (p<0.003). Chylous fistula occurred in 3(5.7%) patients in Group I and in no patients in Group II (table 1) (p<0.24). The stage of tumor, operation type, the day when fistula was noticed, daily fistula output, type of treatment, duration of fistula are outlined in table 4.
| 1. Patient | 2. patient | 3.patient | |
|---|---|---|---|
| Sex | Female | Male | Female |
| Age | 45 | 48 | 69 |
| Etiology/ Stage |
PTC (T2,N1a,M0) |
Recurrent PCA (T2,N1b,M0) |
PTC (T3, N1b, M0) |
| Operation carried out | BTT +CND | Complementary thyroidectomy +LFND | BTT+ LFND |
| The day when fistula was noticed | 2. | 2. | 3. |
| Treatment type | TPN+ sandostatin + compressive bandaging + daily wound care | TPN+ sandostatin+ compressive bandaging + daily wound care |
TPN+ sandostatin+ compressive bandaging +daily wound care |
| Daily fistula output(cc) | 800 | 500 | 300 |
| Fistula duration (day) | 20 | 17 | 15 |
| Postoperative complications | Superficial wound infection | Hypocalcemia |
Table 4: Data of patients with chylous fistula.
Harmonic scalpel produces 0.5 mm lateral spread and 1 mm penetration depth, if activated for 5 seconds on minumum. On the other hand elecrocauter produces 1.9 mm lateral spread and 1.9 mm penetration depth, if activated 5 seconds on 20 W [11,12]. The temperature caused by friction is between 50-100°C with HS and 150- 400°C with electrocautery [7].
The HS has been used for cardiac, gynecologic, abdominal, laparoscopic as well as neck surgery because of its ability to access narrow operating fields. Several recent studies evaluating the effect of HS in patients undergoing neck dissection have shown that use of HS reduced intraoperative blood loss and operative time while maintaining similar complication rates when compared to standard surgical techniques [13-16].
Most studies conclude that HS decreases both intraoperative time and blood loss, even in patients undergoing thyroidectomy with CND and LND [17,18].
He et al. reported that using HS in patients undergoing thyroidectomy with CND reduced the operating time by an avarage of 48 minutes compared with conventional technique [19]. In our study, use of HS decreased the operating time on avarage 19 minutes, since conventional method was only used in dissection of left lower neck, parathyroids and nerves (RILN, vagus, accessory, inferior phrenic and hypoglossal).
There is no randomized study investigating the impact of use of HS on development of thorasic duct injury in dissection of left lower neck region in patients with thyroid carcinoma undergoing CND and LFND.
He et al. demonstrated in their prospective randomized study in 105 patients undergoing total thyroidectomy with CND that 2 patients had postoperative chylous leakage [19]. In this study, patients with clinically positive lymph nodes or functional neck dissection were excluded.
Miccoli et al. in their randomized clinical trial comparing the effect of HS with traditional technique in patients with PTC with neck metastases found that HS decreased significantly operative time, postoperative drainage and produced lower lymphatic spillage. There was no difference in complications such as RILN injury and hypoparathyroidsm between two groups [20]. Our study also showed that there is no difference in RILN injury and hypoparathyroidsm rates between the groups.
Development of chylous fistula is a potentially serious complication of neck dissection and seen in 1-5.8% of cases [21,22]. Chylous leakage is a rare but dangerous complication associated with loss of tissue fluid, hypovolemia, electrolyte imbalance, hypoproteinemia, lymphopenia, immunosupression [23,24]. The most common site of trauma to the thoracic duct is along the lenght of the medial wall of the internal jugular vein due to the fact that it’s the most accessible part of the duct for the patients undergoing neck dissection [21]. The course of the cervical portion of the thorasic duct is highly variable.
Key measures for the conservative treatment of chylous fistula include elevation of the head of the patient’s bed, compressive bandaging, suction drainage and nutritional modifications [21]. Total parenteral nutrition was administered to interrupt the lymphatic flow. Nutritional supplements consisting of medium chain triglycerides may be administered, since they are absorbed directly in to the portal system without having to pass through the lymphatic system [21,24].
Nussenbaum suggest that surgery should be performed when chylous drainage exceeds 1000 ml a day for at least 5 days or when leakage continues after 10 days. On the other hand, De Gier et al. have suggested that conservative treatment should not exceed 30 days in patients with low volume chylous fistulas [21]. Complicated fistulas can be treated using negative –pressure wound therapy and ligation of thoracic duct via thoracoscopy [25,26].
The development of chylous fistula increases the length of hospital stay significantly. Santaolalla et al. have found in their retrospective study of 304 patients undergoing neck dissection that the mean lenght of hospital stay was 33.5 days for patients with chylous fistula compared with 12.7 days those without [21]. In our study, the mean length for hospital stay was 20.6 days for patients with chylous fistula.
In patients undergoing LND and CND due to PTC, in the dissection of the region where ductus thoracicus may be present, conventional methods should be preferred to HS. Especially in patients undergoing LND, ductus thoracicus (Figure 2) should be exposed as much as possible and preserved with a careful and gentle dissection and the main neck lymphatics draining to it should be tied with nonabsorbable sutures, which will decrease the risk of the development of chylous fistula.
In conclusion from the current study we definitely conclude that the use of HS significantly decreases the operative time, but unfortunately may increase the risk of development of chylous fistula.