Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Research Article - (2015) Volume 0, Issue 0
Objective: The aim of the present study was to investigate the relationship of the eNOS Glu298→Asp polymorphisms with impaired flow mediated dilatation (FMD) and diastolic dysfunction in Egyptian children with family history of type-2 diabetes Mellitus (DM).
Materials and methods: Brachial artery FMD and echocardiographic study were performed in 80 (mean age, 11.5 ± 2.2 years) Egyptian non-diabetic offspring of patients with DM, and 80 (mean age, 10.6+2.4 years) Egyptian non-diabetic offspring of non-diabetic parents. Analysis of the endothelial nitric oxide synthase gene polymorphism using polymerase chain reaction and restriction fragment length polymorphism. for detection of different genotype variants (Glu/Glu (GG), Glu/Asp (GT) and Asp/Asp (TT) genotype).
Results: Offspring of diabetic parents showed an increase in the frequency of Glu298Asp polymorphisms, significantly higher compared with controls (P<0.0001). The FMD% was significantly correlated with impaired diastolic dysfunction in offspring of diabetic patients (r=0.435 for IVRT and r=462 for E/Em). The Glu298Asp was significantly associated with impaired FMD and elevated E/Em among non-diabetic offspring of diabetic patients (P<0.001 and <0.005).
Conclusion: Glu298Asp polymorphism in the endothelial nitric oxide synthase gene was significantly associated with impaired FMD and diastolic dysfunction in non-diabetic children with family history of diabetes.
Keywords: Endothelial NO synthase; Flow mediated dilatation; Diastolic function
Impaired endothelial function is an initial step in the development of atherosclerosis, and represents an early and reversible step in the vascular disease process. [1]. The measurement of endothelial function can be used as a surrogate marker to assess cardiovascular risk [2,3].
The molecular etiology of coronary atherosclerosis involves interaction of many genes and environmental factors. Nitric oxide (NO) produced by the enzyme endothelial nitric oxide synthase (eNOS), has critical roles in the regulation of vascular homeostasis and prevention of atherogenesis by inhibiting leukocyte, platelet activation and smooth muscle cell proliferation [3]. Homeostasis of the blood vessel is modulated by vascular endothelium via the production of factors regulating vessel tone coagulation state, cell growth, cell death and leukocyte trafficking [4].
Nitric oxide (NO), which is synthesized from L-arginine by the enzyme endothelial nitric oxide synthase (eNOS) is the most important product of endothelial cells. Endothelial nitric oxide synthase (eNOS; NOS3) produces nitric oxide (NO) from L-arginine. NO has diverse physiologic regulatory functions and is involved in smooth muscle relaxation, inhibition of platelet aggregation, immune regulation, neurotransmission and blood pressure regulation [5].
Polymorphisms of eNOS gene were shown to be associated with CAD in some populations. The guanine to thymine (Glu298Asp) polymorphism at position 894 of the eNOS gene (replacement of glutamate (G) by aspartate (T)) is under extensive study and T allele had been described as susceptibility allele for CAD in some studies [6].
Impaired brachial arterial flow-mediated dilation has similarly been shown in first-degree adult relatives of type 2 diabetic patients [3].
We hypothesized that many of the pathophysiological mechanisms that cause atherosclerotic disease may be present in early childhood in children with family history of type 2 diabetes mellitus, and it may be related to NO gene polymorphism.
The objectives of this study were to evaluate endothelial function, as a marker of early vascular disease and its relation to endothelial nitric oxide synthase (eNOS), in a group of children with family history of type 2 diabetes mellitus.
A prospective cross-sectional study was conducted in cardiology department, Zagazig University Hospital. Eighty healthy prepubertal children (mean age, 11.5 ± 2.2 years), with a family history of diabetes (verbal history of diabetes mellitus with medication for control of diabetes) in one or both parents were enrolled in the study. Eighty healthy children and without parental history of diabetes (age, 10.6+2.4 years) constituted the control group. Informed consent from the parent or legal custodian was obtained, and minor assent (for children ages 7 and older) was administered and obtained as well. The study was approved by the local ethical and scientific committee.
Echocardiographic evaluation
Transthoracic echocardiographic examinations were performed with a ViVid 7 Pro (GE Vingmed Ultrasound, Horten, Norway). The patients were studied without sedation while they were lying in the left lateral position. 3-MHz transducers were used in all echocardiographic studies. Left ventricle (LV) systolic functions and LVMI were assessed using M-mode and two-dimensional (2D). Conventional echocardiography measurements were performed according to the recommendations of the American Society of Echocardiography [7]. We measured early (E) and atrial (A) transmitral maximal flow velocities by pulsed-wave Doppler, then, we calculated the ratio E/A. The isovolumic relaxation time was also measured. Tissue Doppler was performed using a 3-MHz transducer.
Early (Em) and late (Am) diastolic peak annular velocities were measured. The ratio of early mitral flow velocity to the early mitral annular velocity (E/Em) was calculated.
Brachial artery flow mediated dilatation (FMD)
We performed imaging studies of the brachial artery (BA) with a high-resolution ultrasound 7 MHz linear-array transducer with a ViVid 7 Pro (GE Vingmed Ultrasound). Anatomic landmarks were noted on the clearest view of the artery, the skin was marked, and the transducer was held in position by a stereotactic clamp. The internal diameter of the BA, from lumen-intima interface on the near and far vascular wall was measured. After assessing baseline diameter, the BA is occluded by inflation of the cuff 50 mmHg above systolic pressure for 5 minutes on the forearm was used to assess vasodilatation. The proportional response of vasodilatation (i.e. [BA diameter after the test - initial diameter of the (BA)/initial diameter of the BA] and reported as a percentage value (% FMD) [8].
Fasting blood samples were drawn by venipuncture in the morning immediately after endothelial function testing. Blood was sent for laboratory testing including high sensitivity C-reactive protein (CRP), glucose, and serum lipid concentrations.
Analysis of Glu298→Asp polymorphism in exon 7 of the eNOS gene
Genomic DNA was extracted from samples of whole blood by standard methods [9]. The Glu298→Asp polymorphism was a G→T substitution at nucleotide position 894 in exon 7 that encodes for replacement of glutamic acid by aspartic acid at residue 298 in the mature eNOS protein. Genotyping of all participants was by PCR amplification of exon 7 with the primers 5′-CATGAGGCTCAGCCCCAGAAC-3′ (sense) and 5′-AGTCAATCCCTTTGGTGCTCAC-3′ (antisense) followed by MboI restriction enzyme digestion for 16 h at 37 °C. In the presence of a T at nucleotide 894, which corresponds to Asp298, the 206-bp PCR product is cleaved into two fragments of 119 and 87 bp. The products of the digestion process were separated by electrophoresis on a 1.5% agarose gel and visualized by ethidium bromide staining and visualized by ultraviolet light transillumination for determination of Glu298 → Asp endothelial nitric oxide synthase genotypes.
Collected data were computerized and analyzed using the Statistical Package for Social Science (SPSS) version 16. Descriptive statistics were used to describe variables; percent, proportion for qualitative variables, mean SD and range for Quantitative variables. Sampling was performed according to Cai and Zeng [11]. Comparison between groups was done using the Chi-Square test for qualitative variables, independent t-test and ANOVA test for quantitative variables. Pearson correlation was done between two quantitative variables to test association between variables.
The demographic data were summarized in Tables 1 and 2. All data were comparable except serum levels of high sensitivity CRP level was significantly elevated in those with family history of diabetes (P<0.01). Echocardiographic assessment revealed that the isovolumic relaxation time (IVRT) and E/Em ratio were significantly higher in children with family history of DM compared with those without (P<0.05 and <0.01, respectively), (Table 3a and 3b). FMD% were significantly lower in children with family history of diabetes compared with controls (P <0.001), (Table 4). Among children with family history of diabetes, FMD was negatively correlated with IVRT (r=−0. 435; P<0.001) and E/Em ratio (r=−0.462; P<0.015), (Figures 1 and 2).
| Variable | Children with diabetic parents N=80 | Children with diabetic parents N=80 | P-Value |
|---|---|---|---|
| Age (years) | 11.5 ± 2.2 | 10.6+2.4 | >0.05 |
| Gender (males %) | 52.50% | 58.70% | >0.05 |
| BMI (kg/m2) | 22.7 ± 1.6 | 21.5 ± 1.7 | >0.05 |
| WC (cm) | 76.2 ± 9.5 | 73.6 ± 10.1 | >0.05 |
| Mean SBP (mmHg) | 102.5 ± 7.3 | 102.6 ± 7.1 | >0.05 |
| SBP index | 0.86 ± 0.05 | 0.85 ± 0.05 | >0.05 |
| Mean DBP (mmHg) | 66.5 ± 4.5 | 65.8 ± 5.1 | >0.05 |
| DBP index | 0.80 ± 0.6 | 0.79 ± 0.06 | >0.05 |
Table 1: Demographic characteristics of children with and without family. History of diabetes. BMI: Body Mass Index; WC: Waist Circumference; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; LDL: Low Density Lipoprotein; HDL: High Density Lipoprotein; CRP: C-Reactive Protein.
| Variable | Children with diabetic parents (N=80) | Children with diabetic parents (N=80) | P value |
|---|---|---|---|
| Total cholesterol (mg/dL) | 168.5 ± 33.2 | 154.5 ± 31.7 | >0.05 |
| Triglycerides (mg/dL) | 82.2 ± 41.2 | 71.5 ± 42.5 | >0.05 |
| LDL-c (mg/dL) | 90.7 ± 30.5 | 85.6 ± 35.2 | >0.05 |
| HDL-c (mg/dL) | 42.5 ± 13.5 | 46.1 ± 11.5 | >0.05 |
| Glucose (mg/dL) | 85.2 ± 25.3 | 79.8 ± 24.0 | >0.05 |
| Nitric oxide µmol/L | 86.20+9.52 | 43.38+4.15 | <0.001 |
| ET-1 (µmol/L) | 33.75+3.64 | 11.80+2.38 | <0.001 |
| Hcy (µmol/L) | 15.91+3.35 | 10.72+2.15 | <0.01 |
| CRP (mg/dl) | 5.8 ± 2.5 | 1.2 ± 1.6 | <0.01 |
Table 2: Biochemical parameters among both groups.
| (a) Variable | Children with diabetic parents N=80 | Children with non-diabetic parents N=80 | P-value |
|---|---|---|---|
| Left atrial diameter | 2.1 ± 0.4 | 2.2 ± 0.4 | >0.05 |
| Ejection fraction% | 76 ± 12 | 75 ± 13 | >0.05 |
| IVRT(ms) | 58 ± 9 | 52 ± 11 | <0.05 |
| E/A ratio | 1.33 ± 0.35 | 1.42 ± 0.40 | >0.05 |
| E/Em (mean) | 11.2 ± 0.3 | 7.5 ± 0.3 | <0.01 |
| (b) Variable | r | 95% CI | P value |
| FMD% | 4.315 | 1.542-6.951 | 0.001 |
| Left atrial diameter | 0.911 | 0.685-1.692 | >0.05 |
| Ejection fraction | 0.935 | 0.646-1.715 | >0.05 |
| IVRT (msec) | 2.743 | 0.925-3.932 | <0.01 |
| E/A | 1.05 | 0.950-1.782 | >0.05 |
| E/Em | 3.145 | 1.371-6.126 | <0.005 |
Table 3a and 3b: Echocardiographic parameters among both groups. IVRT=Isovolumic relaxation time. Multivariate regression analysis revealed the FMD concentration (r=-4.315; P=0.001); IVRT (r=2.743; P<0.01) and E/Em ratio (r=3.145; P=0.005) as independent factors associated with Glu/Glu polymorphism.
| FMD parameters | Children with FH of DM | Children without FH of DM | *P value | **P value | ||
|---|---|---|---|---|---|---|
| Males (n=42) | Females (n=38) | Males (n=47) | Females (n=33) | |||
| Pre-occlusion flow (ml/min) | 23.5 ± 0.7 | 21.2 ± 0.8 | 12.7 ± 2.3 | 13.5 ± 1.4 | 0.262 | <0.001 |
| Pre-occlusion diameter (mm) | 4.1 ± 0.1 | 4.0 ± 0.1 | 3.9 ± 0.1 | 3.8 ± 0.1 | 0.475 | <0.03 |
| Post occlusion change in diameter (mm) | 0.22 ± 0.3 | 0.22 ± 0.2 | 0.45 ± 0.3 | 0.45 ± 0.2 | 0.679 | 0.01 |
| FMD (%) | 5.4 ± 0.4 | 5.7 ± 0.7 | 11.9 ± 0.8 | 12.3 ± 0.7 | 0.4526 | 0.001 |
Table 4: Flow-mediated dilatation in children with and without family history of type-2 diabetes mellitus. *P: Comparison between male and female. **P: Comparison between offspring of diabetic parents versus those with non-diabetic parents.
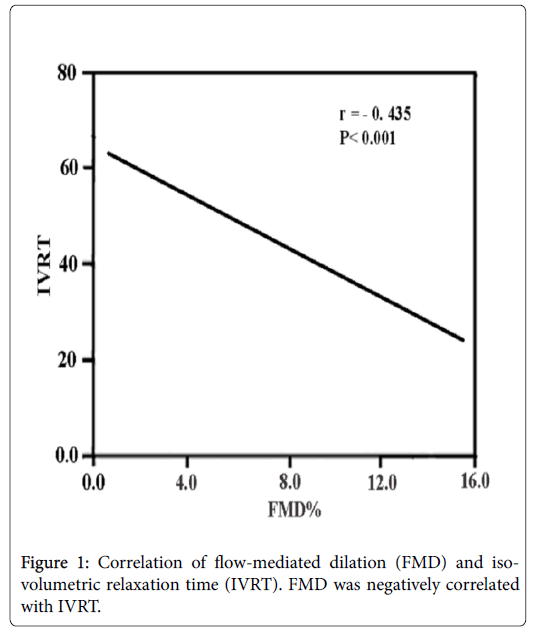
Figure 1: Correlation of flow-mediated dilation (FMD) and isovolumetric relaxation time (IVRT). FMD was negatively correlated with IVRT.
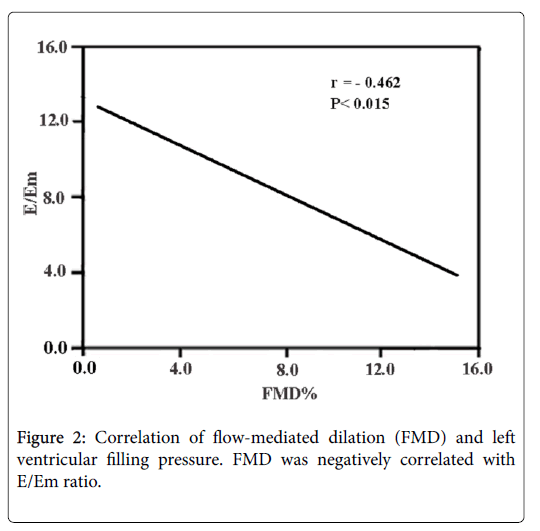
Figure 2: Correlation of flow-mediated dilation (FMD) and left ventricular filling pressure. FMD was negatively correlated with E/Em ratio.
In offspring of family history of diabetes, 30.0% of them were Glu/Glu (GG) genotype, 55.0% were Glu/Asp (GT) genotype and 15.0% were Asp/Asp (TT) genotype, while in offspring of non-diabetic parents, 66.25% of were Glu/Glu genotype, 31.25% were Glu/Asp genotype and 2.5% were Asp/Asp genotype (Table 5).
| Children with FH N=80 | Control N=80 | |||
|---|---|---|---|---|
| eNOS298G > T genotypes | n (%) | 95% CI | n (%) | 95% CI |
| GG | 24(30.0) | 26.9-49.0 | 53 (66.25) | 46.5-67.6 |
| GT | 44 (55.0) | 34.7-57.3 | 25 (31.25) | 26.8-47.3 |
| TT | 12 (15.0) | 9.5-26.5 | 2 (2.5) | 2.4-12.9 |
| p value | 0.003*/0.001** | |||
| Alleles | N=160 | N=160 | ||
| G | 92 (57.5) | 52.3-68.1 | 131 (81.9) | 68.6-81.7 |
| T | 68 (42.5) | 31.9-47.7 | 29 (18.1) | 18.3-31.4 |
| p value | <0.001 | |||
Table 5: Genotype and allele frequency in children with, versus those without family history of type 2 diabetes. *p value<0.003 for comparison among all eNOS. 298G > T genotypes in non-diabetic offspring of diabetic versus nondiabetic parents. **p value<0.001 for comparison between eNOS 298GG and TT genotypes in children with, versus those without family history of type 2 diabetes.
For the 298G >T polymorphism, the frequencies of the 298TT genotype and 894Tallele were significantly higher in offspring with diabetic parents than those with non-diabetic parents (P<0.001), (Table 6). Multivariate regression analysis revealed the FMD concentration (r=-4.315; P=0.001); IVRT (r=2.743; P<0.01) and E/Em ratio (r=3.145; P=0.005) as independent factors associated with Glu/Glu polymorphism (Table 7).
| Children with decreased FMDN=62 | Children with normal FMDN=18 | P value | ||
|---|---|---|---|---|
| GG | N | 22 | 14 | |
| % | 35.8 | 77.8 | <0.001 | |
| GT | N | 35 | 4 | |
| % | 59.14 | 12.2 | <0.001 | |
| TT | N | 5 | 0 | |
| % | 8.06 | 0 | <0.001 | |
| Total | N | 62 | 80 | |
| % | 100 | 100 |
Table 6: Genotype in children with family history of DM with, versus those without decreased brachial artery flow-mediated dilatation.
| Variable | r | 95% CI | P value |
|---|---|---|---|
| FMD% | 4.315 | 1.542-6.951 | <0.001 |
| Left atrial diameter | 0.911 | 0.685-1.692 | >0.05 |
| Ejection fraction | 0.935 | 0.646-1.715 | >0.05 |
| IVRT (msec) | 2.743 | 0.925-3.932 | <0.01 |
| E/A | 1.05 | 0.950-1.782 | >0.05 |
| E/Em | 3.53 | 1.52-5.4 | <0.005 |
Table 7: Multivariate regression analysis of the association between echocardiographic measures and NO polymorphism.
The difference of 24.4% in the frequency of the 894T allele between offspring with diabetic parents and those with non-diabetic parents had 95% power at a level of statistical significance p<0.03.
The Glu298Asp was significantly associated with impaired FMD among non-diabetic offspring of diabetic parents (TT+GT vs. GG OR=3.78 (CI: 1.67-5.9), p<0.0001).
The current study showed that FMD was significantly impaired in offspring of diabetic parents compared to those without family history of diabetes mellitus. The heterozygous and homozygous Asp mutants were significantly associated with the impaired flow-mediated dilatation in non-diabetic offspring of diabetic patients. The GT genotype was significantly correlated with impaired FMD in offspring of diabetic patients. Moreover the decreased FMD% was associated with diastolic dysfunction in offspring of patients with diabetes mellitus. To our knowledge there is no data regarding the association of gene polymorphism and endothelial function in offspring with family history of diabetes. The interpretation of our central finding could be that in type 2 diabetes, the pathophysiological alterations that lead to micro- and macrovascular disease associated with myocardial dysfunction started early in childhood period without any overt metabolic disease.
It was observed that, there was an interaction between the G894T SNP and the cholesteryl ester transferase TaqI B allele was implicated in an increased risk for diabetes in a case-control study carried out in western Iran [11].
Interestingly, endothelial dysfunction may precede the development of diabetes mellitus. In this regard, healthy non-diabetic subjects who have a first degree relative with Type 2 diabetes mellitus display impaired endothelium-dependent vasodilatation as well as increased plasma markers of endothelial cell activation [12,16]. Blood markers of endothelial activation and systemic inflammation are also elevated in non-diabetic offspring with evidence of insulin resistance by glucose tolerance test [12]. Prospective studies have shown that blood markers of endothelial activation predict incident Type 2 diabetes mellitus after adjusting for other risk factors, including body mass index, level of physical activity, lipids, family history of diabetes mellitus, and glucose tolerance [14,15]. Similarly, impaired flow-mediated dilation and polymorphisms of endothelial NO synthase (eNOS) are multivariable predictors of incident Type 2 diabetes mellitus [16]. The occurrence of endothelial dysfunction prior to the development of Type 2 diabetes mellitus suggests that there are common pathophysiological mechanisms and raises that possibility of a causal link between insulin resistance and endothelial dysfunction [17].
Glu298Asp polymorphism of endothelial nitric oxide synthase gene is one of the genetic marker for atherosclerosis that has been extensively studied across the world. The Glu298 → Asp Endothelial Nitric Oxide Synthase gene polymorphism, with the substitution of G by T (replacement of glutamate by aspartate) at nucleotide position 894 in exon 7 reduces the activity of the enzyme, thereby resulting in a decrease in the production of nitric oxide [18,19]. Therefore, the Glu298Asp polymorphism may predispose the individual to an increased risk for atherosclerosis and its complications. There have been conflicting reports on the relationship between this polymorphism and coronary artery disease, functional changes in the endothelium and carotid intima-media thickness (cIMT) from studies done in various ethnic groups across the world [19].
Irma et al. [20] showed that Asp allele occurred more frequently in the subgroups of CAD patients: diabetes mellitus, smoking, hypertension, family history of coronary artery disease and dyslipidemia.
Arterial stiffening in children has recently been found to be associated with nitric oxide synthase 3 polymorphism [21]. Offspring of parents with type 2 diabetes have a high risk of developing diabetes and atherosclerotic complications. Studies have shown increased aortic [22] and carotid-radial, pulse wave velocity in normoglycaemic who are offspring of parents with type 2 diabetes. Impaired brachial arterial flow-mediated dilation has similarly been shown in first-degree adult relatives of type 2 diabetic patients examined the relation between the Glu298Asp polymorphism of the endothelial nitric oxide synthase gene and FMD and found that although there was no relation between the polymorphism and endothelial function in the whole cohort, the 298Asp allele appeared to predispose to endothelial dysfunction in smokers.
Clinical implication
Given the growing relevance of cardiovascular and metabolic disease in this group of children. Understanding the determinants of early disease progression, based on objective measures of vascular phenotype, provides an opportunity for effective, evidence based preclinical intervention.
Limitation
There are some limitations of our study. The first one is the sample, which is probably small for a genetic study. Moreover we have to examine the association of other SNPs of eNOS gene with endothelial function.
Conclusions
The current study identified a clear role of the eNOS gene Glu298Asp polymorphism in impaired flow-mediated dilatationin non-diabetic offspring of diabetic parents. The genetic variants have a positive correlation with impaired FMD and diastolic dysfunction, that promote the development of late cardiovascular diseases.