Medicinal & Aromatic Plants
Open Access
ISSN: 2167-0412
ISSN: 2167-0412
Research Article - (2016) Volume 5, Issue 5
Background: To assess the potential phytoestrogenic effect of Amphimas pterocarpoides plant extract on the ovariectomy (OVX) induced bone loss in rats. Methods: Thirty nine female (10 month old) Wistar rats were separated into Controls (n=11), OVX (n=13) and OVX+AP groups (n=15). Measurements of Bone Mineral Density (BMD) were performed at baseline, 3 and 6 months after ovariectomy. After 6 months treatment, the rats were euthanized and femurs were extracted. The biomechanical properties were evaluated using the 3-point bending test. Results: The percentage changes of the mean values of the proximal tibia BMD from baseline to 3 months for Control, OVX and OVX+AP group were 6.25%, -21.82% and - 12.73% whereas at 6 months they were 8.108%, -32.134% and -22.410% respectively. The 3-point bending test revealed that the maximal load before fracture and the mean values for stress significantly increased in the treatment group compared with OVX rats. Body and uterine weights were similar between OVX and OVX+AP groups. Conclusion: This study is the first to demonstrate that orally administered Amphimas pterocarpoides extract for 6 months is effective in terms of improving bone quantity (Bone mineral density) and quality (biomechanical parameters), surrogate markers of reduced risk of fracture. Therefore, Amphimas pterocarpoides is a new class of phytoestrogen extract and it presents a remarkable antiosteoporotic activity. These properties make Amphimas pterocarpoides a promising herbal therapy for the prevention of postmenopausal osteoporosis induced by estrogen deficiency.
Keywords: Osteoporosis; Rats; Ovariectomy; Phytoestrogens; Bone mineral density; Three point bending
Osteoporosis which is derived from the Greek word meaning porous bone, is defined as a skeletal disease that is marked by low bone mass and structural deterioration of bone tissue, leading to disruption of bone strength and increased bone fractures [1]. Osteoporotic fractures increase a patient’s morbidity and compromise quality of life by causing chronic pain, reduced mobility, depression and finally loss of independence [2].
The public health burden of osteoporotic fractures is likely to rise in future generations due to the increase in life expectancy [3]. One in every two women and one in four men over 50 will have an osteoporosisrelated fracture at some point in their lifetime. It is estimated that 50% of the women who do experience a hip fracture will spend a portion of their recovery in a long term care facility [2]. Therefore, osteoporosis constitutes a major public health problem with implications that cross social, medical and economic lines.
Surgical or natural menopause is the dominant cause of osteoporosis in women because of estrogen deficiency and results in an increased rate of bone turnover and rapid bone loss caused by an imbalance between formation and resorption phases of bone metabolism [4]. Hormone replacement therapy (HRT) has been the first line therapy for the prevention and treatment of osteoporotic fractures in women younger than 60 years or within 10 years of menopause [5]. However, clinical data showed that long term use of conventional HRT is associated with various side effects, including increased risk for endometrial or breast cancer and cardiovascular diseases, which outweighs any benefit [6].
Increasing numbers of experimental studies suggest that estrogen-like compounds of plant origin such as phytoestrogens, have bone preserving effects following ovariectomy [7,8]. Phytoestrogens are comprised of isoflavones, lignans, coumestanes, flavonoids and stilbenes and they present structural and biological similarities with 17-β estradiol, as they can mimic or modulate the actions of endogenous estrogens in target organs by binding both alpha (ERα) and beta (ERβ) estrogen receptors [9].
Various preperations of Amphimas pterocarpoides (AP), a large deciduous tree belonging to the family of Leguminosae, are traditionally used for the treatment of several conditions such as abortion, dysmenorrhoea and impotence, mainly on empirical grounds, and little was known so far about its composition and its properties [10,11]. Based on a recent phytochemical analysis of AP extract, our team detected the presence of 11 different isoflavonoids with strong estrogenic activity [12,13]. To date, there is no scientific report for the anti-osteoporotic properties of AP despite the abundance of isoflavonoids included in it. Therefore, we tested the potential beneficial influence of Amphimas pterocarpoides methanol extract on the prevention of bone loss caused by estrogen deficiency in the ovariectomized rat model.
Animals
The experimental protocol was approved by the General Directorate of Veterinary Services of the Prefecture of Athens (authorization number: 262/13-01-2011), according to Greek legislation (Presidential Decree 160/1991, in compliance with the European Economic Community Directive 86/609/, and Law 2015/1992, in conformance to the European Convention for the protection of vertebrate animals used for experimental or other scientific purposes, 123/1986). Ten-monthold virgin female Wistar rats (n=39) with a mean body weight of 293.5 g were purchased by the registered breeding unit of the Foundation of Biomedical Research of the Academy of Athens. The OVX rat is a well established animal model for studying early postmenopausal bone loss and the age of 10 months is regarded to be the age in which rats reach the peak of their bone mass [14,15]. The animals were housed four together in transparent polycarbonate cages (45 × 30 × 20 cm; IFFA) with wood chip bedding (Rehofix MK2000, Germany). In addition, they were acclimated under standard laboratory conditions with a 12-h dark/light cycle, controlled temperature ranging between 19°C and 22°C, light intensity of 300 Lux measured one meter above the floor in the middle of the room, relative humidity 55-65% and 15 air changes/ hour. The rats were given a soybean-free rat diet (Diete Speciali 4RF21 modified, Italy) after ovariectomy.
Rats were divided into three groups (Figure 1), by allocating littermates to each group, in order to avoid genetic and anatomical variations among them. After 7 days of acclimatization in this laboratory environment, all rats were subjected to Bone Mineral Density (BMD) measurements using dual-energy X-ray absorptiometry (DEXA) and transferred to the operation theatre, where they were either shamoperated (Control) or ovariectomized (OVX). Control (n=11) and OVX (n=13) rats received drinking water ad libitum right after surgery until the end of the experiment, while the remaining ovariectomized rats were administered Amphimas pterocarpoides extract at 50 mg/ kg (AP+OVX, n=15). The extract was orally administered in their drinking bottles starting one day after surgery. Due to the 6 months treatment duration, per οs gavage was avoided as being stressful to the animals. Drinking water intake of animals was pre-evaluated and its substitution by the Ampimas pterocarpoides extract did not influence that consumption. Water and extract consumption was applied ad libitum and was recorded twice a week. The bottles were shaken several times daily to avoid the accumulation of precipitate. All rats were weighed during the experimental period on a weekly basis and examined daily.
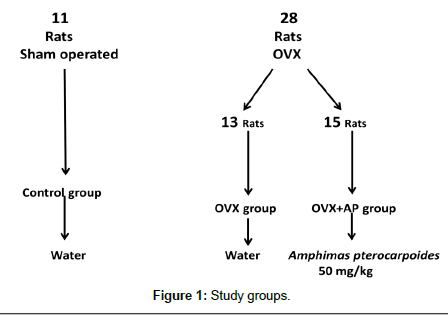
Figure 1: Study groups.
To minimize the increase in bodyweight caused by ovariectomy, the food consumption of ovariectomized rats was adjusted weekly according to the level of Control rats consumption. Measurements of BMD of proximal and total tibia were performed at baseline, 3 and 6 months by the same experienced operator. At the end of 6 months, all rats were anesthetized (ketamine at 10 mg/kg, xylazine 3 mg/kg im) and euthanized after exsanguination from the abdominal aorta. Necropsy followed in order to identify possible malignancies or other pathological findings. The uterus was dissected, cleaned of fat tissue and weighed immediately using a high accuracy electronic analytical balance scale (Sartorius handy H60, H110). Success of ovariectomy was confirmed by failure to detect ovarian tissue and observation of marked atrophy of the uterine horns. Vital organs and abdominal fat were also removed and weighed. The femurs were isolated, cleaned of soft tissues and wrapped in normal saline soaked gauze to prevent dehydration and frozen at -20˚C according to the best method of long-term preservation before biomechanical testing [16]. The flow-chart of the experiment is presented in Figure 2.
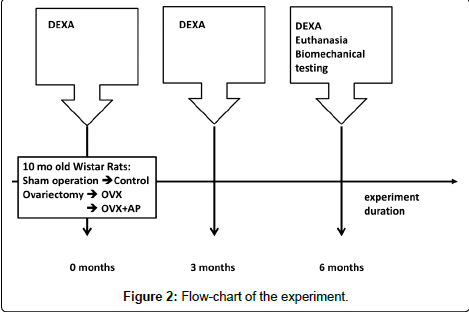
Figure 2: Flow-chart of the experiment.
Plant material
Collection, extraction and HPLC-DAD analysis: The stem barks of Amphimas pterocarpoides were collected at Mount Eloumdem, in the suburbs of Yaounde, Center Region of Cameroon, in March 2010 and authenticated by Mr. Victor Nana, botanist at the National Herbarium of Cameroon where a voucher specimen is conserved under the reference number 52563/HNC. The material was dried under shade and ground using a flour mill. Furthermore, a methanol extract was produced as follows: 10 kg of the powder obtained from the stem bark of Amphimas pterocarpoides were extracted with methanol of analytical grade and the extract was concentrated under reduced pressure at 40°C giving a residue which in turn was lyophilized to produce a final material of 348.5 g (3.48% yield). HPLC-DAD analysis of the extract was performed using a Thermo Finnigan apparatus (Thermo Finnigan, San Jose, CA) equipped with two P4000 pumps, a degasser, an autosampler, a DAD, and a system controller. A Discovery SUPELCO HS C-18 column (25 × 4.6 mm i.d., 5 μm particle size) was used for the separation of peaks while the system was similarly controlled by ChromQuestTM 4.1 software. A binary mobile phase gradient with a flow rate of 1 mL/min was incorporated for the assay. 1% aqueous acetic acid (solvent A) and methanol (solvent B) were used. A simple linear gradient program of 2% B to 98% B in 90 min was developed, followed by an isocratic step of 98% B. These conditions were kept for 5 min before returning to initial condition of 2% B, which were also kept for 5 min for re-equilibration of the system between individual runs. Figure 3 represents the HPLC chromatogram of AP recorded at 254 nm. Several peaks characterized as polyphenolic compounds could be resolved and the 11 previously isolated isoflavonoids were also identified in this extract.

Figure 3: HPLC-DAD profile of a methanol extract of the stem bark of Amphimas pterocarpoides at 254 nm.
Ovariectomy: Animals were weighed and anesthetized (ketamine 70 mg/kg, xylazine 3 mg/kg) by intramuscular injection before surgery. Using aseptic procedures, bilateral OVX was performed through a midline ventral incision for OVX and OVX+AP groups. The ovaries were dissected and removed by cutting above the ligation. Peritoneum and skin were stitched separately in layers by single interrupted sutures. The same procedures were followed for the Control group, except that the ovaries were identified but not removed. Peri and postoperative care included administration of enrofloxacin (Baytril 5% 10 mg/kg) for three days and carprofen (Rimadyl 0.08 ml/kg) subcutaneously the operation day and the following.
Bone mineral density: Measurements of BMD of the total and proximal tibia of the rats were established by DEXA at baseline, 3 and 6 months using Lunar Prodigy Advance Densitometer machine equipped with Small Animal Scan Software. The anesthetized rats were positioned in the middle of the measurement table and scans obtained in a high resolution mode. Total tibia BMD was evaluated by inclusion of the whole tibia in the region of interest (ROI). For the evaluation of trabecular bone BMD, a square ROI of 2 × 2 mm2 was selected in the proximal tibial metaphysis, 3 mm distal to the tibial plateau. The in vitro precision (coefficient of variation) of the system was 0.5%. The system was calibrated before every group measurement.
Biomechanical testing: In order to evaluate the mechanical properties of rats femoral bones, three point bending (3PB) tests were implemented using an electromechanical loading frame (MTS Insight 10 kN). On the day of the experiments, the femoral bones were removed from the storage at -20°C, thawed and held at room temperature at least for an hour before the procedure, a process that has proven not to cause significant changes in the mechanical characteristics of the specimens. Each specimen was photo-graphed front and back and if any remarkable anatomical observation was noted, the specimen was excluded.
The femurs were placed horizontally on two supports of rounded edges 20 mm apart, always in the same manner based on anatomical characteristics of the bone in an effort to minimize scattering factors (Image 1a). In the case of improper placement, specimens were excluded from the study. Then the load was imposed on the diaphysis midshaft in the anterior-posterior layer using a punch of rounded notch. A very small pre-load was applied in order for the specimen to be stabilized on the supports and then two points were marked on the specimen corresponding to the specimen-punch contact point and the respective one at the lowest side of the specimen at the same vertical line with the previous one. This procedure was necessary for the loading axis to be known after the specimen’s fracture.

Image 1: Biomechanical testing procedure.
The tests were quasi-static under displacement-control mode at a rate equal to 1 mm/min. The load was imposed monotonically until the bone’s fracture. The quantities measured during the tests were the load imposed, the displacement of the frame’s traverse and the deflection of the bone’s mid-section. The latter was achieved in a non-contact manner using a video extensometer (RTSS HR Video Extensometer, Limess) with a sampling rate of 1 Hz. The data were recorded through TestWorks programs 4.
In the second phase of the experimental procedure, the mechanical strength of each specimen was determined in terms of the bending fracture stress. The latter is considered as the most reliable index of the bone’s strength since it does not depend on the size of the cross section of each specimen. For this to be accomplished, the exact geometric features of the cross section of each specimen had to be determined as close as possible to the fracture section. In this direction the part of each fractured specimen corresponding to the lateral condyle of femur was properly placed in molten resin Versocit-2 (Struers) and Epofix (Struers) (Image 1b). After solidification of the resin the surface of the bone-resin complex was properly polished by Labopol 5 (struers) to acquire the exact form of the cross section (Image 1c). The inner and outer contours of the cross section were then digitized with the aid of a suitable stereoscope (Image 1d).
Taking advantage of these contours and using the Solid Works software the following characteristics of the fracture cross section were determined: The geometrical center of the cross section, the cross section’s area, the mean and minimum thickness of the cross section and the second order moments of the cross section with respect to the principal centroidal system. In addition (and knowing the direction of the loading axis) it was possible to determine also the bending neutral line, the eccentricity of the loading axis with respect to the section’s geometrical center and finally the most heavily stressed point of the cross section’s outer contour. Given this information it was possible to calculate the fracture stress by adopting the technical bending theory by Bernoulli-Euler.
Statistical analysis
Continuous variables are presented with mean and standard deviation (SD). Quantitative variables are presented with absolute and relative frequencies. For the comparison of study variables between the Control, OVX and OVX+AP groups, the analysis of variance (ANOVA) was used. Bonferroni correction was used in order to control for type I error, in multiple testing. Differences in changes of total tibia and proximal tibia BMD during the follow up period between the three study groups were evaluated using repeated measurements ANOVA. All p values reported are two-tailed. Statistical significance was set at 0.05 and analyses were conducted using SPSS statistical software (version 19.0).
The sample consisted of 39 Wistar rats (11 in the Control group, 13 in the OVX group and 15 in the OVX+AP group). Table 1 presents changes in total tibia and proximal tibia BMD during the observation period for the three study groups. At baseline, total tibia BMD was similar between the three groups. At three and six months, total tibia BMD was greater in the Control group as compared with the two other groups. During the follow up, the total tibia BMD remained unchanged for the Control group, while a significant reduction was found for OVX and OVX+AP groups both from baseline to three months and from three to six months. The mean percentage reduction of total tibia BMD from baseline to six months was -10.73% for the OVX group and -11.32% for the OVX+AP group (Table 1). The mean percentage reduction of total tibia BMD from three to six months was -5.01% for the OVX group and -3.04% for the OVX+AP group (Table 1).
| Total Tibial | Baseline | 3 months | 6 months | % change from baseline to 3 months | % change from baseline to 6 months | % change from 3 to 6 months | P** Baseline vs 3 months | P** Baseline vs 6 months | P** 3 months vs 6 months |
P‡ |
|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) (g/cm2) |
Mean (SD) (g/cm2) | Mean (SD) (g/cm2) | Mean (SD) | months | Mean (SD) | |||||
| Control a | 0.213 (0.011) | 0.215 (0.012) | 0.217 (0.011) | 1.043 (2.876) | 1.684 (3.447) | 0.634 (1.939) | 0.800 | 0.405 | 1.000 | <0.001 |
| OVX b | 0.213 (0.009) | 0.200 (0.006) | 0.190 (0.007) | -6.016 (2.646) | -10.727 (3.720) | -5.011 (2.997) | <0.001 | <0.001 | <0.001 | |
| OVX+AP c | 0.217 (0.010) | 0.199 (0.008) | 0.193 (0.007) | -8.526 (3.015) | -11.321 (2.779) | -3.039 (1.451) | <0.001 | <0.001 | <0.001 | |
| P * a vs b | 1.000 | <0.001 | <0.001 | |||||||
| P * a vs c | 0.841 | <0.001 | <0.001 | |||||||
| P *b vs c | 0.651 | 1.000 | 1.000 | |||||||
| Proximal Tibial | ||||||||||
| Control a | 0.331 (0.022) | 0.351 (0.018) | 0.357 (0.017) | 6.254 (3.392) | 8.108 (3.125) | 1.793 (3.040) | 0.001 | <0.001 | 0.630 | <0.001 |
| OVX b | 0.330 (0.023) | 0.258 (0.031) | 0.224 (0.024) | -21.822 (7.035) | -32.134 (5.905) | -12.900 (6.907) | <0.001 | <0.001 | <0.001 | |
| OVX+AP c | 0.345 (0.018) | 0.301 (0.011) | 0.267 (0.017) | -12.731 (3.971) | -22.410 (5.532) | -11.101 (4.716) | <0.001 | <0.001 | <0.001 | |
| P * a vs b | 1.000 | <0.001 | <0.001 | |||||||
| P *a vs c | 0.301 | <0.001 | <0.001 | |||||||
| P *b vs c | 0.185 | <0.001 | <0.001 |
*group effect comparisons after Bonferroni correction
**time effect comparisons after Bonferroni correction
‡time * group effect
Groups: (OVX) ovariectomy, (OVX+AP) ovariectomy plus Amphimas pterocarpoides extract, (Control) sham operated.
Table 1: Changes in primary outcome measures during the follow up period for the three study groups.
Proximal tibia BMD at baseline was similar between the three study groups. At three and six months, proximal tibia BMD was greater in the Control group as compared with the two other groups and greater for the OVX+AP group as compared with the OVX group. A slight increase was found for the proximal tibia of the Control group, while in the two other groups proximal tibia decreased significantly both from baseline to three months and from three to six months. The mean percentage reduction of proximal tibia from baseline to three months was greater for the OVX group in comparison with the OVX+AP group (-21.82% vs. -12.73%, p<0.001, Table 1). Also, a greater reduction in proximal tibia was found for the OVX group in comparison with the OVX+AP from baseline to six months (-32.13% vs. -22.41%, p<0.001).
The mean values of biomechanical parameters for the three study groups are shown in Table 2. Force was significantly lower in the OVX group as compared with the Control group (p=0.024). Furthermore OVX+AP demonstrated significantly greater values in contrast to OVX group (p<0.001). Stress was significantly greater in the OVX+AP group as compared with the OVX group (p=0.005). Additionally, stress was significantly lower in the OVX group as compared with the Control group (p=0.011).
| Group | ||||
|---|---|---|---|---|
| Controla | OVXb | OVX+AP c | ||
| Mean (SD) | Mean (SD) | Mean (SD) | P Anova | |
| Force (N) | 110.8 (12.14)b | 96.9 (11.74)a,c | 112.69 (12.41) b | <0.001 |
| Stress (Mpa) | 179.68 (11.84)b | 158.48 (13.78)a,c | 180.5 (11.84)b | 0.003 |
Note: a, b, c indicates significant differences (p<0.050) after Bonferroni correction.
Groups: (OVX) ovariectomy, (OVX+AP) ovariectomy plus Amphimas pterocarpoides extract, (Control) sham operated.
Table 2: Mean values of biomechanical parameters for the three study groups.
Table 3 presents the mean final body weight, organs and abdominal fat weight for the three study groups after the 6 month treatment period. Significantly smaller mean values, of body weight were found in the Control group in comparison with the OVX (p=0.015) and OVX+AP (p=0.004) groups. Significantly greater mean values of the uterus were found in the Control group in comparison with the OVX (p=0.002) and OVX+AP (p=0.021) groups. Also, mean fat values were significantly greater in the OVX (p=0.044) and OVX+AP (p=0.001) groups in comparison with the Controls.
| Body weight (gr) | Group | P | ||
|---|---|---|---|---|
| Controla | OVXb | OVX+APc | ||
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| 330.91 (33.33)b.c | 377.08 (35.84)a | 383.5 (42.27)a | 0.003 | |
| Brain | 1.99 (0.08) | 1.97 (0.12) | 1.97 (0.08) | 0.801 |
| Heart | 0.86 (0.12) | 0.89 (0.10) | 0.89 (0.10) | 0.795 |
| Kidney | 0.78 (0.09) | 0.79 (0.09) | 0.82 (0.12) | 0.656 |
| Liver | 7.68 (1.08) | 7.35 (1.64) | 8.41 (0.79) | 0.081 |
| Uterus | 0.42 (0.09)b,c | 0.15 (0.03)a | 0.22 (0.27)a | 0.002 |
| Fat | 21.56 (4.53)b,c | 29.72 (7.75)a | 34.53 (7.10)a | <0.001 |
Note: a, b, c indicates significant differences (p<0.05) after Bonferroni correction
Groups: (OVX) ovariectomy, (OVX+AP) ovariectomy plus Amphimas pterocarpoides extract, (Control) sham operated.
Table 3: Comparison of the mean values of bodyweight, abdominal fat and organ weights among groups.
Osteoporosis is the most serious bone remodeling disease which is characterized by low bone mass and high risk of fractures. It is well documented that estrogen deficiency is an important risk factor in the pathogenesis of osteoporosis. Although, HRT is an established therapeutic option for postmenopausal bone loss, recent evidence indicate that its long term use is related to side effects such as the increased risk of endometrial and breast cancer [5]. Thus, alternative treatments are under investigation. To our knowledge, despite the abundance in isoflavonoids in AP extract, no scientific data of its antiosteoporotic properties have been published to date. Our study is the first to demonstrate that Amphimas pterocarpoides extract consumption is safe, has potent effects on trabecular bone BMD, ameliorates the deterioration of bone mass and improves biomechanical properties in the ovariectomized rat model of osteoporosis.
Monitoring of BMD using DEXA is considered as the gold standard for the assessment of people who are at risk to develop osteoporosis. The decrease in bone mass is a major characteristic of osteoporosis and DEXA analysis best predicts the fracture risk in people without known history [17]. Our results indicate that total and proximal tibia BMD were significantly decreased in the OVX group at 3 and 6 months after ovariectomy in contrast to Control group, a fact which confirmed the influence of estrogen deficiency on bone mass. Furthermore, the present study demonstrated that rapid bone loss in rats following ovariectomy occurred in a site specific fashion. In three months time, the BMD reduction in proximal tibia (-21.822%) was greater than the reduction of total tibia BMD (-6.016%) in the OVX group. This is due to the fact that, bone composition differs between the regions of long bone. Total tibia consists primarily of cortical bone which is regarded to be less affected by ovariectomy, while the proximal tibia on the other hand is dominated by trabecular bone which is more prone to bone turnover [18]. It is well documented that estrogen deficiency in rats leads to permanent and significant loss of trabecular bone in only two weeks time [14,19]. Indeed, in our experiment the BMD values obtained from the tibias showed that the strong counter acting effect of AP on bone loss at three months was observed at the trabecular compartments of the proximal tibia. In the OVX+AP group, the percentage reduction of BMD in proximal tibia from baseline was -12.731%, indicating the AP protective effect, while in the cortical compartments of the total tibia the percentage reduction was -8.526%, similar to the non-treated OVX animals. The cortical bone rich regions which is included in the ROI measurements does not suffer such a dramatic loss in the early post OVX [19,20]. The mean percentage reduction of the proximal tibia BMD from baseline was greater for the OVX group in comparison to the OVX+AP group (-21.82% vs. -12.73%, p<0.001), demonstrating that AP plant is effective in preventing the onset of osteoporosis taking place during the first three months after ovariectomy. Moreover, a greater reduction in proximal tibia was found for the OVX group in comparison with the OVX+AP from baseline to six months (-32.13% for the OVX group vs. -22.41% for the OVX+AP group, p<0.001), indicating that extract consumption continued its protective effect (Table 1). Our findings are in keeping with data from previous studies with phytoestrogens in Wistar rats, that confirmed their bone protective effect [21,22].
On the other hand, our study demonstrated no differences between OVX and OVX+AP group in total tibia BMD absolute values and their percentage change from baseline to 3 and 6 months time. However, between three and six month time, the mean percentage reduction of total tibia BMD was greater for the OVX group (-5.011%) compared to the OVX+AP group (-3.039%) (p<0,001), indicating a mild protective effect of Amphimas pterocarpoides on cortical bone turnover. The discrepancy observed in the time effect of ovariectomy on bone density in the total tibial, is explained by the late effect of estrogen deficiency on cortical bone, requiring at least 3 to 4 months time before changes become obvious [14,18].
The occurrence of a fracture depends not only on bone mass and density but also on bone structure and architecture [18,23,24]. Biomechanical analysis is a reliable way to evaluate bone quality through studying the mechanical properties of bone tissue under external action and give us valuable knowledge regarding the integrity of bone function [16]. Furthermore, biomechanics allow us to identify the biological effects of bone under force or stress [23]. Previous studies have proved that although low bone mass in osteoporotic bones is a major risk factor for the occurrence of a fracture, the presence of adequate trabecular microstructure can preserve the biomechanical properties of the bone [25,26].
In our study, OVX resulted in statistically significant decrease of trabecular BMD and reduction of long bone’s biomechanical strength (Tables 1 and 2). At the end of 6 months period, in the OVX group less maximum force and ultimate stress were required for fracture to occur compared to the Control group (Table 2). In the OVX+AP group, trabecular BMD was preserved and biomechanical properties were accordingly maintained. Maximum force and the stress applied were significantly higher in the OVX+AP compare to the OVX group. The present study confirmed the beneficial effect of AP extract on both the bone quantity (bone density) and quality (biomechanical parameters), surrogate markers of reduced risk of fracture [27]. Similar studies with skeletally mature rats and oral administration of plant extracts from Achyranthes bidentata, Sideritis euboea, Eucommia ulmoides oliv. at higher doses, demonstrated improved biomechanical properties of the femora through modification of BMD [19,28,29].
Moreover, our study suggested an acceptable safety profile of the AP on top of the implied therapeutic effect. Estrogen therapy is known to cause hyperplasia of the uterus and it is strongly associated with malignancies both in uterus and breast, as a result of their undesirable non selective action [30,31]. The AP extract did not significantly increase the uterus weight and no cancer was detected with autopsy after 6 months of treatment in our study group. The action of isoflavones contained in the extract mimics the action of estrogens in target organs and is mediated by binding to both alpha (ERα) and beta (ERβ) estrogen receptors (ER). ERβ are more than ERα in bone tissue, while ER-α appear mainly in breast and uterus [32]. The lack of action of the AP extract on the uterus might be explained by a higher affinity of the extract for ERβ than ERα.
A meta-analysis from Fu et al. demonstrated the protective effect of phytoestrogens in the estrogen-deficient rats by preventing the reduction of BMD [8]. Based on previous experimental studies, oral administration of plant extracts should begin right after OVX, especially for phytoestrogens with mild estrogenic action, due to the fact that changes in proximal tibia post OVX are clearly evident in 2 weeks time [15,28,29,33]. The beneficial effect of AP extract on the prevention of bone loss and maintenance of bone strength after ovariectomy might be related to the presence of different types of isoflavonoids included in it. Based on recent data, conducted by HPLC, eleven isoflavonoids were isolated from the methanol extract of the stem bark of AP [12]. Some of these isolated isoflavonoids such as daidzein, clycitein and formononetin have proven anabolic effect on bone metabolism and they prevent bone loss [20,32,34-37]. A good correlation between the content of AP extract in isoflavones and its antioxidant activity has already been described [10,11] while the role of oxidative stress in the pathogenesis of osteroporosis is well established [38,39].
At the end of the observation period of our study, the body weights of the ovariectomized animals, irrespective of receiving treatment or not, were significantly higher than those of the Control group, although all animals had the same calory intake. In addition, a predominant abdominal fat deposition was observed at necropsy and increased abdominal fat weights were measured in both ovariectomy groups. Weight gain, with abdominal predominance, is a well known consequence of menopause, is related to estrogen deficiency and probably mediated by the decreased production of estradiol and the subsequent lack of ERα activation [40,41]. Even though obesity seems to protect bones by stimulating neoformation, it remains an unwanted effect due to its implication in the development of cardiovascular disease or cancer [42,43]. The AP extract in the present dose failed to inhibit the rise in body weight in our study, but this might be a doserelated effect. Furthermore experimental data indicate that bone is more sensitive to isoflavones than the uterus and adipose tissue [44].
In conclusion, the oral administration of Amphimas pterocarpoides plant extract for 6 months in estrogen deficient ovariectomized rats can prevent bone loss and it contributes to the preservation of trabecular bone mineral density, thereby maintaining structural integrity, as well as contributes to the biomechanical competence of the bone. Furthermore, our results clearly demonstrate that this extract from AP stem bark had no hypertrophic effect on the uterus. Therefore, Amphimas pterocarpoides extract could be considered as an attractive natural alternative anti-osteoporotic herbal treatment. More experimental studies are needed to clarify its precise mechanism of action, as well as clinical data regarding its use in the prevention of postmenopausal osteoporosis.
IKY fellowships of excellence for post graduate studies in Greece-Siemens programme, for the conduction of the experimental protocol. The International Foundation of Science is acknowledged for their contribution to the ethnobotanical study and the collection of Amphimas pterocarpoides through the grant F/3336-2F to Dieudonné Njamen.
Anastasia Patsaki and Job Tchoumtchoua have equally authorship for the present work and should be regarded as co-first authors.