Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2014) Volume 3, Issue 3
Background: Hepatotoxicity is historically the 3rd most common reason for ART toxicity related discontinuation. Liver toxicity leads to medical visit, work plan exams, and frequent hospital admissions all of which increases expenses. The objective of this study was to determine the risk of hepatotoxicity and identify the major predictors that may cause hepatotoxicity in the study place.
Methods: A case-control study was done by reviewing a total of 105 TB/HIV co- infected patients' charts.
Results: Of the total 105 patients included in the study, 21 (20%) developed hepatotoxicity. Fifty four (51.43%) of the participants were females. The mean CD4 count of the patients was 205.1 + 96.18 cells/μL and ranged from the lowest count of 51cells/μl to the highest recorded count of 559cells/μl. The most frequent anti-TB regimen prescribed was 2(INH, RIF, ETM, PZA)/4(INH, RIF). Ninety five (90.5%) of the participants were on the primarily prophylactic drugs. Of this figure, 49 (46.7%) were on cotrimoxazole. Number of female patients developed hepatotoxicity were 12 (57.1%). Most of the patients who had developed hepatotoxicity were in stage 3 of HIV/AIDS progression. Social drug use was significantly associated with development of hepatotoxicity (P=.005) with a 95% CI (0.01-311). Patients on TDF/3TC/EFV (OR= 121.7, P=.010) and D4T/3TC/NVP (OR= 47.4, P=.009) ART regimen were found to be more likely to develop hepatotoxicity compared to patients on D4T/3TC/EFV regimen. Similarly patients on 2(ERHZ)/4(RH) anti-TB regimen (OR= 575.96, P=.002) with a 95% CI (0.02-3.8), was found to be more likely to develop hepatotoxicity compared to the other types anti-Tb regimens.
Conclusions: The risk of hepatotoxicity in TB/HIV coinfected patients can be due to a number of factors among which sex, the WHO clinical staging, use of Social drugs, type of ART regimen and type of anti-TB regimen are the major, according to the findings of this study.
<Keywords: Risk of Hepatotoxicity; HIV/TB Co Infection; Adama Referral Hospital
Worldwide, it is estimated that 14.8% of all new tuberculosis (TB) cases in adults are attributable to Human Immunodeficiency Virus (HIV) infection. This proportion is much greater in Africa, where 79% of all TB/HIV co infections are found [1]. The advent of Highly Active Antiretroviral Therapy (HAART) in the treatment of HIV infection has significantly decreased the incidence of opportunistic infections as well as improved morbidity and mortality among HIV patients [2]. However, along with these positivity outcomes, HAART is associated with a number of adverse reactions [3]. Drug-Induced Hepatotoxicity (DIH) is one of the overlapping side effects of both Anti-Retroviral Therapy (ART) and first line anti-TB drugs leading to interruption of treatment [4,5].
Hepatotoxicity is historically the 3rd most common reason for ART toxicity related discontinuation [6]. The most important risk factors for hepatotoxicity in individuals receiving TB treatment are: Age >35 years; being a child; perhaps a female gender; Hepatitis B surface Antigen (HBsAg) positive; use of alcohol; slow acetylator status; extensive TB disease; increase in baseline ALT; malnutrition; Hepatitis C Virus (HCV) co infection; and HIV co-infection [6]. Other cause includes co-administered medications like cotrimoxazole and anti-fungals [7-9].
When Hepatotoxicity implies that the liver shows an elevation in Serum Aspartate Amino Transferase (AST) or Alanine Amino Transferase (ALT) level from the normal range (AST = 0-37 and ALT< 41 IU/l) to >3x upper limit of normal in the presence of symptoms, or Serum AST or ALT greater than 5 times the upper limit of normal in the absence of symptoms [1,10]. AST/ALT elevations instead of Alkaline Phosphatase (ALP) elevations favor liver cell necrosis as a mechanism liver cholestasis. When AST and ALT are both over 1000 IU/L, the differential can include acetaminophen toxicity, shock, or fulminant liver failure. When AST and ALT are >3X of normal but not > 1000 IU/L, the differential can include alcohol toxicity, viral hepatitis, drug induced, liver cancer, sepsis, Wilson disease, post-transplant rejection of liver, autoimmune hepatitis, and steatohepatitis (non-alcoholic). When AST/ALT elevated is minor it may be due to rhabdomyolysis among many possibilities [11]. Therefore, these tests could be used as markers of hepatocellular injury [12]. Hepatocellular injury has different grading scale from mild to severe based on the concentration of the ALT or AST [13,14]. Studies have revealed that 14-20% of adults on ART had elevated serum liver enzymes as a marker of hepatocellular injury [15].
Liver toxicity generates medical visit, work plan exams, and frequent hospital admissions all of which increases expenses. In addition, hepatotoxicity hampers the maintenance of HIV suppressions over time [16]. Thus, the purpose of the present study was to determine the risk of hepatotoxicity in patients treated for TB-HIV co infection using the serum ALT level as the marker of hepatotoxicity.
Study design
A case-control study was conducted by reviewing charts of TB/HIV co- infected patients.
Inclusion and exclusion criteria
All Patients on HAART and TB treatment and on ART follow up clinic of Adama Hospital from 27/7/2011 to 30/3/2014 were included in the study. While patients who had no or had less than three liver function tests, and patients with incomplete records were excluded.
Sample size calculation and sampling method
Sample size was determined using case control sample size formula considering a 4 to 1 control to case proportion. A total of 105 patients were included in the study. A systematic random sampling method was used to select the patients based on ART number of each patient.
Dependent and independent variables
The presence of hepatotoxicity was taken as a dependant variable and other variables such as socio demographic factors, behavioral factors, immunological factors, clinical factor, weight in Kg, ART regimen, start of art, TB disease, other drugs use, anti-TB regimen, primary prophylactic drugs and opportunistic infections were taken as independent variables.
Data organization, presentation and analysis
Data was coded and entered into the Statistical Package for Social Science (SPSS) version 16 for Windows. Figures and tables were used to present findings. Chi-square, Fishers exact tests and binary logistic analysis were used to test for the level of significance. OR and P-values are used to see the significant risk factors. Variables with p<0.05 were considered potential predictors of hepatotoxicity.
Data quality assurance
A 5% sample pretest was performed on randomly selected patients before the beginning of the study. A pretested and validated check list was used. All steps in data collection and recording were closely monitored by the principal investigator and daily collected data was, recorded and compiled for the next day study.
Ethical considerations
Ethical clearance was obtained from the Ambo University ethical review committee and official cooperation was sought and secured from Adama Referral Hospital. Patient consent was not needed because the study was a retrospective study and no personal identity was disclosed to maintain patients’ confidentiality. The raw data was not made available to anyone, and was not used as the determinant of any identity or subjects.
Socio-demographic data
The mean age of the total patients was 37.2 + 13.7 years and ranged from 3-71 years of age (Figure 1). Fifty two (49.5%) of the patients were between age 31-45 years. There were 54 (51.43%) female patients and from these 12 (11.4%) were among the case group and moreover, 71 (67.6%) of the patients were orthodox Christians (Table 1).
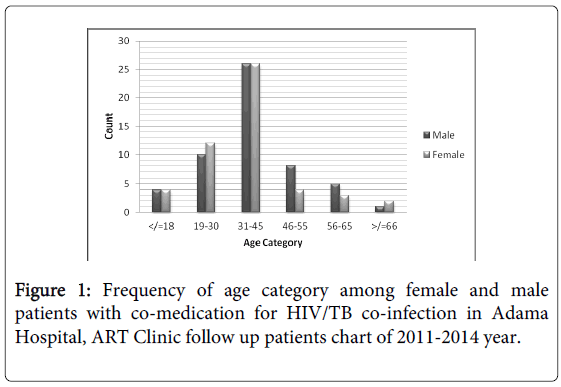
Figure 1: Frequency of age category among female and male patients with co-medication for HIV/TB co-infection in Adama Hospital, ART Clinic follow up patients chart of 2011-2014 year.
| Variables | Cases | Control | Percent | |
|---|---|---|---|---|
| Sex | Female | 12 | 42 | 51.43 |
| Male | 9 | 42 | 48.57 | |
| Age category | 3 | 5 | 7.62 | |
| 19-30 | 2 | 20 | 20.95 | |
| 31-45 | 12 | 40 | 49.52 | |
| 46-55 | 3 | 9 | 11.43 | |
| 56-65 | 0 | 8 | 7.62 | |
| >/=66 | 1 | 2 | 2.86 | |
| Weight Category | Lowest thru 60 | 21 | 77 | 93.33 |
| 61 thru 70 | 0 | 6 | 5.71 | |
| 71 thru 80 | 0 | 1 | 0.95 | |
| Marital Status | Never married | 12 | 31 | 40.95 |
| Married | 4 | 25 | 27.62 | |
| Divorced | 5 | 28 | 31.43 | |
| Religion | Orthodox, Christian | 13 | 58 | 67.62 |
| Protestant, Christian | 4 | 11 | 14.29 | |
| Muslim | 4 | 15 | 18.10 | |
| Educational background | Illiterate | 6 | 9 | 14.29 |
| Primary school | 4 | 18 | 20.95 | |
| Secondary school | 8 | 50 | 55.24 | |
| College/University | 3 | 7 | 9.52 | |
Table 1: Socio-demographic variables of the study participants obtained from Adama Hospital, ART Clinic follow up patients chart of 2011-2014 year.
Fifty eight (55.2%) of the patients’ had reached secondary school while only 10 (9.5%) of the patients had attended college or university level courses. Considering the marital status of the study participants, 43(41%) were never married while only 25 (27.6%) were married (Table 1).
Behavioral characteristics of the study participants
With regard to behavioral characteristics of the study participants 19(18.81%) drank alcohol regularly, where as 10(9.5%) smoked cigarettes and 13(12.4%) used social drugs such khat plant based on the criteria of yes/no question on patient ART follow up chart (Figure 2).
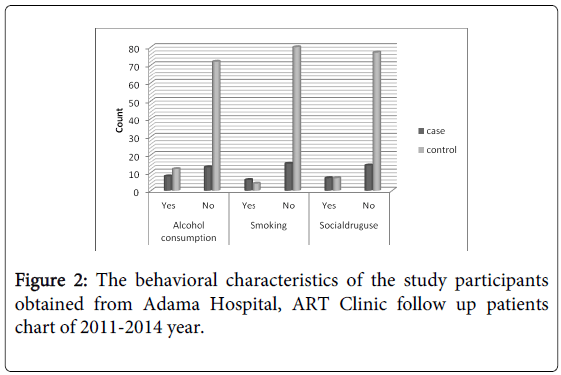
Figure 2: The behavioral characteristics of the study participants obtained from Adama Hospital, ART Clinic follow up patients chart of 2011-2014 year.
Clinical and Immunological characteristics of the patients
The mean CD4 count of the patients was 205.1 + 96.18 cells/µL and ranges from the lowest count of 51 cells/µl to the highest recorded count of 559 cells/µL. Eighty six (83.8%) of the patients had CD4 count less than or equal to 200 cells/mm.
Majority of male patients 28 (26.67%) and female 27 (25.7%) patients were on the WHO clinical stage III. Five patients (4.8%) were on the WHO stage I (Figure 3). Six (5.3%) were positive for HBsAg and only 4 (3.8%) were positive for anti-HCV.
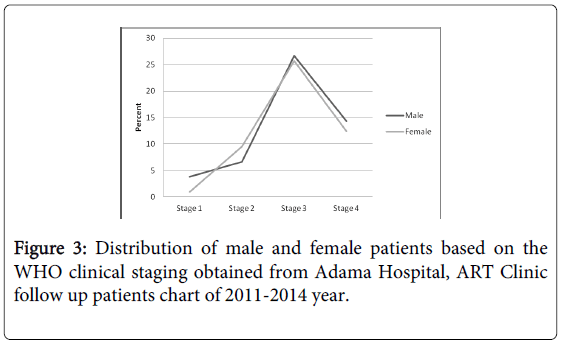
Figure 3: Distribution of male and female patients based on the WHO clinical staging obtained from Adama Hospital, ART Clinic follow up patients chart of 2011-2014 year.
Out of the total recruited patients 72 (68.6%) had pulmonary tuberculosis and 29 (27.6%) had extra pulmonary TB and only 4 (3.8%) had disseminated TB.
Eighty (76.2%) of the participants started ART simultaneously with TB treatment. But 16 (15.2%) of the participants started ART previous to TB treatment. Only 9 (8.6%) of the study participant started ART after completion of TB treatment. Among the cases started ART previous to TB treatment 6 (28.6%) developed Grade 2 hepatotoxicity. But majority of the patients who developed hepatotoxicity were patients that start their ART simultaneous to TB treatment and only 2 (9.5%) of patients who took their ART after TB treatment developed hepatotoxicity (Figure 4).
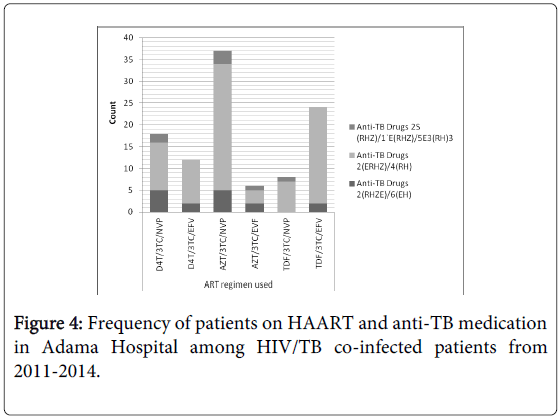
Figure 4: Frequency of patients on HAART and anti-TB medication in Adama Hospital among HIV/TB co-infected patients from 2011-2014.
With regard to ART regimen used, 37 (35.1%) of the participants were on AZT/3TC/NVP and 6 (5.7%) were on AZT/3TC/EFV. Eighteen (17.1%) and 12 (11.4%) of participants were on d4T/3TC/ NVP and d4T/3TC/EFV respectively. The remaining patients were on TDF based combination therapy, 8 (7.6%) on TDF/3TC/NVP and 24 (22.9%) on TDF/3TC/EFV.
The most frequent anti-TB regimen prescribed was 2 month (INH, RIF, ETM, PZA)/4month (INH, RIF) with 13 (61.9%) and 82 (78.1%) in cases and controls respectively. In the case group the second most frequent regimen was 2 month (INH, RIF, ETM, PZA)/ 6month (INH, ETM) 6 (28.6%). Ninety five (90.5%) of the participants were on the primarily prophylactic drugs. Of this figure, 49 (46.7%) were on cotrimoxazole, 39 (37.1%) were on INH and 7 (6.7%) on fluconazole. Generally, the prevalence of opportunistic infections was 94 (89.6%).
Among TB cases 71 (67.6%) were pulmonary type and 29 (27.6%) were extra pulmonary type. Six (28.6%) patients with pulmonary TB, 13 (61.9%) patients with extra pulmonary and 2 (9.5%) patients with miliary type TB had developed Grade 2 hepatotoxicity. The most frequent type of TB among the control group was pulmonary tuberculosis while the predominance type of TB among the cases was extra pulmonary TB (Figure 5).
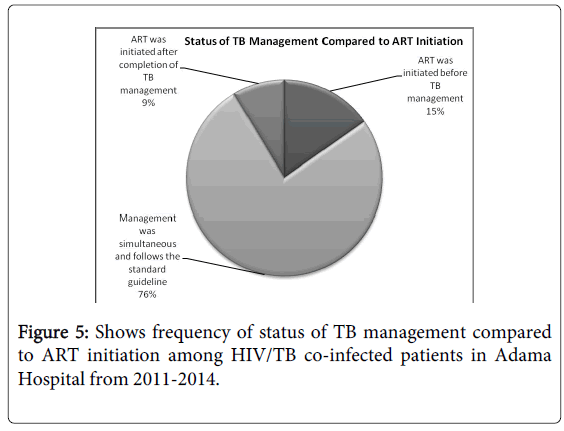
Figure 5: Shows frequency of status of TB management compared to ART initiation among HIV/TB co-infected patients in Adama Hospital from 2011-2014.
Determinants of Hepatotoxicity among HIV/TB Co-Infected Patients
Hepatotoxicity was common among patients on primary level of education (p=0.1). Similarly, those patients who were put on AZT/3TC/NVP (P=0.009) and TDF/3TC/EFV (P=.01) were significantly associated with ALT elevation. Patients with extra pulmonary TB (p=0.001) were more likely to develop hepatotoxicity among HIV/TB co-infected patients. Moreover, 2 months (ERHZ)/ 4month (RH) anti-TB regimen was significantly associated with ALT elevation. As expected, patients on social drugs use were found to be associated with the development of hepatotoxicity (P=.005) with a 95% CI (0.01-311).
The toxicity grade as per the WHO’s criteria, majority was toxicity grade zero 84 (80%). The whole patients on the case group developed toxicity grade 2 based on ALT measurements of patients on co-medication for HIV/TB infections (Figure 6). Moreover, spearman correlation analysis showed that there was no association between hepatotoxicity based on ALT measurements with age, weight and/or CD4 count.

Figure 6: Shows Grade of toxicity based on ALT test result of patient on co-medication for HIV/TB infection.
Patients on TDF/3TC/EFV and D4T/3TC/NVP ART regimen were found to be 121 and 47 times more likely to develop hepatotoxicity respectively compared to patients on D4T/3TC/NVP regimen (OR= 47.4, P=.009). Moreover, it was common in patients on anti-TB regimen of 2 months (ERHZ)/4 months (RH) with [P=.002; 95% C.I .02-3.8] (Table 2).
| Variables | Case | Control | % | df | Sig. | AOR | 95.0% C.I for AOR | ||
|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||
| Educational level | Illiterate | 6 | 9 | 14.3 | 3 | 0.38 | --- | ||
| Primary school | 4 | 18 | 21.0 | 1 | 0.1 | 0.004 | 0.000 | 0.877 | |
| Secondary school | 8 | 50 | 55.2 | 1 | 0.449 | 2.27 | 0.242 | 77.03 | |
| College/University | 3 | 7 | 9.5 | 1 | 0.320 | 0.23 | 0.592 | 161.8 | |
| Type of ART regimen used | D4T/3TC/NVP | 4 | 14 | 17.1 | 5 | 0.127 | --- | ||
| D4T/3TC/EFV | 5 | 7 | 11.4 | 1 | 0.116 | 9.8 | 0.003 | 2.2 | |
| AZT/3TC/NVP | 7 | 30 | 35.2 | 1 | 0.009** | 47.4* | 0.000 | 0.314 | |
| AZT/3TC/EVF | 0 | 6 | 5.7 | 1 | 0.998 | 0.00 | 0.030 | 5.1 | |
| TDF/3TC/NVP | 2 | 6 | 7.6 | 1 | 0.358 | 4.43 | 0.000 | ||
| TDF/3TC/EFV | 3 | 21 | 22.9 | 1 | 0.010** | 121.7* | 0.001 | 1.2 | |
| Type of TB diagnosis | Pulmonary | 6 | 66 | 68.6 | 2 | 0.002 | --- | ||
| Extra pulmonary | 13 | 16 | 27.6 | 1 | 0.001** | 0.003 | 0.021 | 0.1 | |
| Miliary | 2 | 2 | 3.8 | 1 | 0.297 | 0.12 | 0.000 | 970 | |
| Tb drugs regimen | 2(RHZE)/6(EH) | 6 | 10 | 2 | 0.005 | --- | |||
| 2(ERHZ)/4(RH) | 13 | 69 | 78.1 | 1 | 0.002** | 576.96* | 0.002 | 3.823 | |
| 2S(RHZ)/1`E(RHZ)/5E3(RH)3 | 2 | 5 | 6.7 | 1 | 0.201 | 12.4 | 1.617 | 13.3 | |
| Social drug use | Yes | 7 | 7 | 13.3 | 1 | 0.005** | 0.021 | 0.001 | 311 |
| No | 14 | 77 | 86.7 | 1 | 0.203 | 0.13 | |||
Table 2: Multiple Logistic Regressions result of patients of HIV/TB co-infected patients in Adama Hospital Medical College from 2011-2014.
In the present study a total of 105 patients’ were recruited retrospectively and among which 21 (20%) developed hepatotoxicity. Hepatotoxicity was confirmed based on laboratory criteria of 3 consecutive ALT measurements of >3X the Upper Limit of Normal (ULN) in the presence of clinical pictures of DILI and ALT measurements of great than 5 times the ULN in the absence of sign and symptoms. This finding is higher compared to a study conducted in Sweden and another study in Ethiopia [5,17] and still this figure is much higher than the 6% report from Tanzania [18]. These variations could be due to the fact that our study participants were all patients co-infected with TB/HIV and could also be due to the difference in sample size. Further, the majority toxicity grade as per the WHO’s criteria, was toxicity grade zero 84 (80%) unlike of other similar study conducted in Ethiopia [5].
In our study, 86 (83.8%) of the patients had CD4 count less than or equal to 200 cells/mm, this result is in line with other similar study [19]. The mean CD4 count of the patients was 205.1 + 96.18 cells/µL and ranges from the lowest count of 51 cells/µl to the highest recorded count of 559 cells/µl. Furthermore, there were 54 (51.43%) female patients participated in the study and this record also similar to other previously conducted study [19]. Twelve (57.1%) female patients developed hepatotoxicity based on the laboratory criteria of 3 consecutive ALT measurements. Female sex consideration in hepatotoxicity is important because pregnancy and related gynecological disorders could affect the incidence and the tolerability to DILI. Majority of male patients 28 (26.67%) and female 27 (25.7%) patients were on the WHO clinical stage III, which is similar to study conducted in Ethiopia (71.4%) [5].
The reported incidence of HAART and/or anti-TB DILI can be associated with a number of factors. We investigated the risk of hepatitis B and C virus infection in patients infected with HIV and TB, and 6 (5.3%) were positive for HBsAg and only 4 (3.8%) were positive for anti-HCV and this result was also comparable to other similar study [19]. However, we did not observe effect of hepatitis B or C co-infection was a significant risk factor for DILI, similar to the study conducted in Jimma, Ethiopia [17]. However, many studies are reporting that there are significant association between DILI and these viral infections. The reason could be due to lack of routine lab tests in the study area in association with unavailability and patient economic issue.
Most of the patients who had developed hepatotoxicity were on WHO clinical stage 3, same as to the study conducted in Sweden and Ethiopia [17,18]. Debilitation from the hepatotoxicity, HIV and TB could possibly have impact on the immune response as well as the metabolism of the drugs. Therefore, it could be these reasons that put the majority of the patients in stage III. Social drug use was significantly associated with development of hepatotoxicity in our study (OR=P=.005) with a 95% CI (0.01-311), but we could not found article matching our results. Considering the direct toxicity of these medications as well as their impact on the mental status of the patients, they could possibly have a significant effect on adherence of anti-TB/ART medications.
Patients on TDF/3TC/EFV (P=0.010) and AZT/3TC/NVP (P=0.009) developed hepatotoxicity 121.7 times and 47.2 times respectively, compared to patients on D4T/3TC/NVP. This figure could be due to the fact that nowadays many of HIV patients are being treated with AZT, D4T and ABC based regimen than D4T based regimen. The reason has been clarified as severe ADR reaction encountered up on prolonged use of the medication. And similarly patients on 2(ERHZ)/4(RH) anti-TB regimen with (P=.002) and a 95% CI of (0.02-3.8), were investigated to develop hepatotoxicity 575.96 times more frequently than the other types of anti-Tb regimens. These findings were also in line with other studies conducted in different part of the world [17-19].
Our investigation based on spearman correlation analysis showed that, no statistical association between developing hepatotoxicity in TB/HIV co-infected patient on medications with age, weight and/or CD4 count. This finding was also similar to other study [17].
Clinical records are usually not complete. The study also addresses past circumstances and has a limitation of representativeness, because the study was conducted only in one hospital.
The risk of hepatotoxicity in TB/HIV coinfected patients can be due to a number of factors among which sex, the WHO clinical staging, use of Social drugs, type of ART regimen and type of anti-TB regimen are the major, according to the findings of this study. However, the study also showed that there was no statistical correlation between hepatotoxicity with age, weight and/or CD4 count.
The authors’ are grateful to Ambo University College of Medicine and Health Sciences and department of Pharmacy, Adama Hospital admin and health staffs, and patients for their direct and indirect participation and unreserved support for the success of this study.
The following WHO operational definitions were used in the study:
Toxicity of degree 0: the level of toxicity which is considered as normal in which its value is <1.25 x normal value of ALT in serum
Toxicity of degree 1: the Level of toxicity which is considered as weak in which its value is 1.256 – 2.5 x normal value of ALT in serum
Toxicity of degree 2: the Level of toxicity which is considered as moderate in which its value is 2.6 – 5 x normal value of ALT in serum
Toxicity of degree 3: the Level of toxicity which is considered as severe in which its value is 5.1 – 10 x normal value of ALT in serum
Toxicity of degree 4: the Level of toxicity which is considered as severe in which its value is >10 x normal value of ALT in serum
Category I anti-Tb drugs: Initial Phase (8 weeks) with INH, RIF, PZA, EMB and Continuation Phase (26 weeks) with INH/RIF or INH/RPT
Category II anti-Tb drugs: Initial Phase (8 weeks) with INH, RIF, PZA, EMB and Continuation Phase (26 weeks) with INH/RIF or INH/RPT
Category III anti-Tb drugs: Initial Phase (8 weeks) with INH, RIF, PZA, EMB and Continuation Phase (26 weeks) with INH/RIF
Category IV anti-Tb drugs: Initial Phase (8 weeks) with INH, RIF, EMB and Continuation Phase (39 weeks) with INH/RIF