Journal of Molecular Imaging & Dynamics
Open Access
ISSN: 2155-9937
ISSN: 2155-9937
Case Report - (2017) Volume 7, Issue 2
Introduction: Kikuchi-Fujimoto disease (KFD), also known as Kikuchi’s disease or histiocytic necrotizing lymphadenitis, is a self-limiting case of non-cancerous lymphadenopathy. Although previous reports have demonstrated its physical findings and traditional imaging characteristics, few studies mentioned the application of 18fluorodeoxyglucose positron emission tomography-computed tomography (18F-FDG PET/CT) imaging in the diagnosis and follow-up of this disease. Here, we present three cases of KFD, describe the findings from PET/CT images and review the relevant literature to improve the diagnosis of this rare disease.
Case presentation: Three patients, two females (15 and 16 years old) and one male (28 years old), with KFD were diagnosed by biopsy. All patients presented with bilateral cervical lymph nodes and no history of fever, and underwent multiple physical examinations, conventional imaging (Ultrasonography, CT and MRI) and 18F-FDG PET/CT. The images from 18F-FDG PET/CT revealed increased FDG uptake in all three patients. We also observed that the maximum standardized uptake value (SUVmax) in the affected lymph nodes in our patients ranged from 4.85 to 21.1 (mean ± SD, 10.53 ± 3.02) and the mean of SUVmax values ranged from 3.5 to 17.3 (mean ± SD, 7.35 ± 4.13), while 12 out of 16 large nodes with the maximum values of SUVmax were located in the cervical region. All patients presented with splenomegal which showed low affinity to FDG.
Conclusion: Our study showed that 18F-FDG PET/CT imaging of KFD was mainly characterized by mild-tomoderate FDG uptake on the affected lymph nodes with maximum diameter of less than 35 cm and no or mild lymph node fusion and rarely extra-nodal infiltration. Moreover, 18F-FDG PET/CT may be a useful tool in the diagnosis of KFD prior to biopsy; where location, size and the response to FDG may be the important and useful factors for making clinical decision for biopsy.
Keywords: FDG PET/CT; Kikuchi-Fujimoto disease (KFD); Histiocytic necrotizing lymphadenitis
Kikuchi-Fujimoto disease (KFD) also known as Kikuchi’s disease or histiocytic necrotizing lymphadenitis, is a self-limiting clinical condition of non-cancerous lymphadenopathy. The disease was first described in 1972 by two Japanese scientists Kikuchi and Fujimoto [1-3]. KFD is more prevalent in the Asian nations than in the western world. It is a rare disease that presents predominantly in young woman in their 20’s and 40’s.
The disease is of acute or sub-acute onset and clinically progressive. It is characterized by fever which is commonly associated with viral infection, leukopenia and atypical lymphocytes which are frequently observed in the peripheral blood, lymph node swelling mostly in the posterior cervical triangle, and unresponsiveness to antibiotics treatment. Its definitive diagnosis is usually made by biopsy.
We analyzed three patients diagnosed to have KFD and who underwent conventional imaging (US, CT or MRI) and molecular imaging (PET/CT). Initially the patients underwent a low-dose CT acquisition with 120 kV, 60 mA, at a speed of 22.5 mm/s, without any specific breath-holding instructions. Without changing the patient’s position, PET scans were then carried out after acquisition of the CT [4,5]. All patients were fasted for 6 h, and PET scans were performed after controlling the blood glucose level below 150 mg/dl. Complete body scanning from the base of the skull to the mid-thigh was performed using the Discovery LS PET/CT system (GE Medical Systems).
Five to seven bed positions were performed each with an acquisition time of 2-3 mins. Reconstruction of PET images was done using an OSEM algorithm. CT data were used for attenuation correction. PET/CT interpretation were performed on the Xeleris workstations (ELGEMS, Haifa, Israel) equipped with fusion software, which enables the display of PET images (with attenuation correction), CT images and fused data of both modalities. Any site of increased FDG uptake on the PET images and showed as lymphoma node at the same position was considered as a possible lymphoma site [6-8].
We performed a comprehensive search of PubMed (including MEDLINE compiled by the United States National Library of Medicine, Bethesda, Maryland, USA) and China bio-medicine databases to identify published original, review articles and case series reporting the KFD. Searches were limited to studies conducted from January 2002 to December 2011.
We used the keywords (“PET/CT” or “position emission tomography-CT” or “18FDG” or “18fluorodeoxyglucose”) and (“KFD” or “Kikuchi-Fujimoto disease” or “Kikuchi's disease” or “histiocytic necrotizing lymphadenitis”) [9-11].
We identified 8 studies through this search strategy. We also handsearched several imaging and immunology journals for the specified period to ensure that the electronic search did not miss reports of eligible studies; but we could not identify additional study through this strategy. We further searched the reference list of the retrieved studies for any additional publications, and none of the articles was found in this approach.
We present here three cases, for which the final histological diagnosis was KFD. All three patients underwent conventional imaging (Ultrasonography, CT or MRI) and PET/CT as described before. Laboratory investigations including blood cells analysis, virus detection (CMV, EBV and COXBV), serum antibodies (ds-DNA) and relevant tuberculosis (including PPD test) investigations were conducted in all three patients. Laboratory and imaging findings are detailed in Table 1. Other imaging and PET/CT findings are shown in Table 2.
| Variables | Case 1 | Case 2 | Case 3 |
|---|---|---|---|
| Age | 16 | 28 | 15 |
| Sex | Female | Male | Female |
| Body temp | Raised | Raised | Raised |
| Lymphadenopathy | +++ | +++ | +++ |
| WBC | 4.5 × 109/ | 3.7 × 109/ | 2.1 × 109/ |
| LP% | 60.50% | 72.70% | 49.80% |
| CRP | 15 mg/L | 20 mg/L | 16 mg/L |
| ESR | 25 mm/h | 23 mm/h | 17 mm/h |
| Virus detection | (+) CMV-IgM | (+) EV-IgM | (+) COXB3-IgM |
| (+) COXB5-IgM | |||
| (+) CMV-IgM | |||
| Antibodies analysis | (-) | (-) | (-) |
| Relevant TB tests | (-) | (-) | (-) |
| Steroid therapy | Effective | Effective | Effective |
| Diagnosis after Biopsy | KFD | KFD | KFD |
| WBC: White Blood Cells; LP%:Lymphocytes Proportionality; CRP: C-Reactive Protein; ESR: Erythrocyte Sedimentation Rate; CMV: Cytomegalovirus; EV:Enterovirus; COX: Coxsackie Virus; (-) – Negative or Absent; (+) – Positive or present | |||
Table 1: Patients’ clinical presentations, laboratory findings and provided treatment.
| Variables | Case 1 | Case 2 | Case 3 |
|---|---|---|---|
| Age | 16 | 28 | 15 |
| Sex | Female | Male | Female |
| Location of cervical nodes | RC: II | RC: III, IV, IV | RC: II, III, IV, V |
| LC: II | LC: II, III, V | ||
| Other nodal sites | Left axilla | Post peritoneum | -- |
| Size of the largest lymph node (cm) | 2.4 × 1.5 | 2.7 × 1.8 | 3.2 × 2.8 |
| Site | Left Axilla | Right cervical | Right cervical |
| Range of nodal diameter (cm) | 0.7-1.3 | 0.7-2.7 | 0.8-3.2 |
| Nodal fusion/matting | No | No | Yes |
| Extra-nodal involvement | No | Yes (hepatic) | No |
| SUVmax | 5.4 | 10.4 | 10.7 |
| Site | Left Axilla | Right cervical | Right cervical |
| Mean of SUVmax | 2.8 | 7.1 | 6.7 |
| Splenomegaly | +++ | +++ | +++ |
| Nodal enrichment | No | No | No |
| Key: SUVmax: Maximum standard uptake value; RC: Right cervical; LC: Left cervical; LA: Left axilla, LC: Left cervical | |||
Table 2: The patients’ characteristics of conventional and PET/CT imaging.
Case 1
A 16-year-old girl presented with a two weeks history of fever of unknown origin and left cervical lymphadenopathy. She had no other complaints. On examination, multiple, mobile, mild tender lymph nodes measuring 0.7-2.4 cm in diameter were palpable on the left cervical region. The patient also had hyperemic nasal pharynx, mild bilateral tonsillar swelling, splenomegaly and no other palpable lymph nodes. CT scan revealed bilateral cervical lymphadenopathy, while other lymph nodes were normal.
The nodes had a uniform central necrosis with no areas of reinforcement, while peripheral nodal infiltration was distinctly visualized as obliteration or increased attenuation of the adjacent fat tissues on contrast-enhanced CT. A whole body 18F-FDG PET/CT revealed multiple enlarged nodes demonstrating FDG-avid bilateral cervical regions (on region II) and left axilla without anastomosis phiphenomenon which measured as standardized uptake value (SUVmax 2.6-5.4) and a non-FDG-avid splenomegaly. Biopsy of the left cervical lymph nodes confirmed the diagnosis of KFD.
On the seventh day after administration of 12 mg/kg dehydrocortisone, fever subsided. After two weeks, the patient was discharged home to continue with the medication. The dose was gradually tapered down and then stopped on the third week of its initiation. On further outpatient follow-up, the patient reported no further symptoms, with obvious decrease in size of the bilateral cervical lymph nodes and no abnormal physical examination.
Case 2
A 28-year-old man presented with a more than one-week history of low-grade fever of unknown origin and right cervical lymphadenopathy with no other complaints. On examination, the patient had body temperature of 38.5, with multiple palpable discrete nodes in the maxilla, posterior, cervical and inguinal regions. A tender, slightly limited mobile lymph node measuring 3.0 cm in diameter was palpable in the right cervical region. The patient also had hepatomegaly. An abdominal CT showed a hypo-dense lamellar focus in the right lobe of the liver, splenomegaly and clusters of lymphadenopathy in extra-peritoneal region and hepatic hilar region.
Nodal necrosis was seen on CT, and showed no contrast enhancement and anastomosis phi-phenomenon. Whole body 18FFDG PET/CT scan revealed multiple nodes demonstrated as FDG-avid masses in the right cervical (on region III, IV and V), the largest lymph node in region IV measuring about 2.7 cm × 1.6 cm in size, and those in the right cervical region with SUVmax measured as 2.5-10.4. There was an abnormal focus in the right hepatic lobe (focus diameter: 1.1 cm; SUVmax 5.7). Discrete and matted lymph nodes were detected in hepatic hilar region and extra-peritoneal areas (SUVmax 4.4-11.6); Biopsy of the right cervical mass confirmed the diagnosis of KFD.
After administration of intravenous Ganciclovir and steroid therapy, there was an obvious decrease in the lymphadenopathy and the patient had normal physical examination.
Case 3
A 15-year-old boy presented with a two-month history of hyperpyrexia, right cervical lymphadenopathy and swollen parotid gland. He had no any other complaints. On physical examination, his body temperature was 39.5, and had hyperemic nasal-pharynx and bilateral tonsillar swelling. On palpation, there was a mobile and mild tender lymph node on the cervical region which measured about 2 cm in diameter. The patient also had palpable multiple lymph nodes in the bilateral axillary and inguinal regions. There was no splenomegaly. CT scan showed a lump in the right parotid gland, enlarged lymph nodes in the bilateral cervical regions and axillary fossa which had uniform central necrosis with no reinforcement on CT; MRI scan displayed multiple nodes with weighted T1 and T2 signals at bilateral cervical regions and axillary fossa. An 18F-FDG PET/CT whole body scan showed multiple FDG-avid and matted nodes in the bilateral cervical regions (on the right side: in regions I, II, III, IV and Vleft sidein regions II, III and V); SUVmax ranged from 4.3 to 10.7 and the highest uptake was seen on the supraclavicular regions which showed SUVmax of 10.4. The scan also showed an FDG-non-avid splenomegaly. Biopsy of the right cervical lymph node confirmed the diagnosis of KFD. Histopathological examination showed a distorted lymph node architecture replaced by extensive necrotic areas, filled with apoptotic bodies. There were no neutrophilic granulocytes (Figure 1).
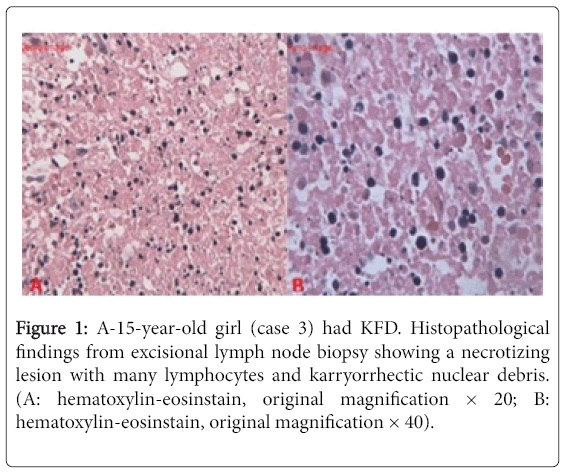
Figure 1: A-15-year-old girl (case 3) had KFD. Histopathological findings from excisional lymph node biopsy showing a necrotizing lesion with many lymphocytes and karryorrhectic nuclear debris. (A: hematoxylin-eosinstain, original magnification × 20; B: hematoxylin-eosinstain, original magnification × 40).
Symptomatic relief was obtained after administration of 40 mg dehydrocortisone. The patient was discharged after three weeks of hospital stay, and Dihydrocortisone dose was gradually titrated and stopped at the third week after discharge.
From the 8 reviewed studies, a total of 13 cases were studied. The characteristics features of the patients and their lesions are summarized in Table 3.
| Patient number | Study, reference | Sex/Age | Lymph nodes | Mean SUVmax | SUVmax | Extra-peritoneal node | Maximum node(mm) | Maximum node site |
|---|---|---|---|---|---|---|---|---|
| 1 | Ito et al. [12] | F/36 | BC/BA/Me | 5.77 | 9.67, RC | - | 13.7x11.8 | LC |
| 2 | Ito et al. [12] | M/23 | BC/BA/Me/I | 4.98 | 10.25, LC | - | 23.4X12.7 | M |
| 3 | Ito et al. [12] | F/31 | LC | 4.9 | 4.9, LC | - | 20.4X11.2 | LC |
| 4 | Ito et al. [12] | F/28 | BC | 3.5 | 4.85, LC | - | 23.8X13.1 | LC |
| 5 | Ito et al. [12] | F/25 | RC | 5.23 | 5.23, RC | - | 17.8X10.8 | RC |
| 6 | Ito et al. [12] | F/43 | RC/BA | 9.87 | 13.94, RA | - | 27.8X14.8 | RA |
| 7 | Ito et al. [12] | F/66 | BC/LA/Me | 7.98 | 12.9, M | - | 18.2X6.9 | LC |
| 8 | Lee et al. [13] | F/8 | BC/BA/I | Mild-to-mode rate uptake | - | + | <30 | RC |
| 9 | Alfred et al. [14] | F/26 | BC/LA/M | Moderate uptake | - | - | <30 | RC |
| 10 | Chung et al. [15] | F/10 | RC | - | - | + | <25 | RC |
| 11 | ShipraKaicker et al. [16] | F/19 | LC/M | 5.7 | 10.5, LC | <20 | LC | |
| 12 | Zhang et al. [17] | F/18 | RC/BA | 10.4 | 17.03, RC | + | 20 | RT |
| 13 | Yasu Yoshida et al. [18] | M/44 | M | 17.3 | 21.1, M | - | <30 | M |
| PET/CT:Position Emission Tomography/Computed Tomography; SUVmax:Maximum Standard Uptake Value; F:Female; M:Male; BC:Bilateral Cervical; RC:Right Cervical; LC:Left Cervical; BA:Bilateral Axilla; RA:Right Axilla; LA:Left Axilla; Me:Mediastinum; I: Inguinal region; RT: Retroperitoneal region | ||||||||
Table 3: Revision of the literature of KFD.
KFD is a self-limiting disorder and non-tumorous hyperplasia of the lymph nodes. Although the disease has a worldwide distribution, it is more prevalent in Asia than in other parts of the world. It is a rare disease that presents predominantly in young woman. The female: male ratio in our cases was as high as 4.3:1, although some previous studies have shown minor or no female preponderance with female: male ratio ranging from 1.1:1 to 2.75:1 [5]. In children, however, there is a completely different male gender predominance where the diseases have been reported to be more prevalent in boys than in girls (male: female = 2.8:1) [8]. The mean age of patients in previous reported studies was 25.5 years old and ranged from 8 to 66 years [8].
There is a lot of debate on the etiology of KFD, however the definitive etiology is yet to be known. Most studies have implicated viral and autoimmune causes as the possible causes of the condition. In recent years, various studies have reported a close association between viral infection such as Epstein-Barr virus, and Cytomegalovirus and the disease. In all three patients reported in our study, the evidence of different viral infections was found in laboratory investigations. The contribution of some other viruses like (HHV6, HHV8, and parvovirus B19) in the pathogenesis of KFD remains controversial and is not very convincing [6].
In one of recent reports, apoptotic process induced by Fas protein was reported to be a significant finding in the viral pathogenesis of KFD [7]. In Table 1 the white blood cell count indicated leukocytopenia while lymphocytosis in the three patients is a further proof of viral infections. Apart from the raised ESR (normal: ≤ 15 mm/h) and CRP (normal: ≤ 8 mg/L) values, other biochemical parameters were all negative. The anti-ENA results and all other investigations for tuberculosis (including PPD test) were also negative. All the three patients were finally diagnosed to have KFD by lymph node biopsy. After several weeks of steroid therapy, all the three patients' clinical conditions improved.
On conventional radiological imaging (US, CT or MRI), the affected lymph nodes in KFD usually appear enlarged and possess an abnormal round shape. In our all three patients, the enlarged lymph nodes were found in the cervical, left axillary and extra-peritoneal regions, most of which appear as small-to medium-sized lymph nodes with maximum diameter rarely exceeding 3.5 cm except for some matted nodes in case 3 (right cervical II).
The affected cervical lymph nodes have a tendency to be located unilaterally or bilaterally at levels II, III and IV and shows areas of low attenuation on CT. Previous authors [4] have reported areas of low attenuation in some lymph nodes were located centrally with a thin peripheral rim around them and areas of obvious necrosis. Peri-nodal infiltration is also frequently found on CT scans. The CT features reported in several other case studies or large scale analytical studies are consistent with what has been reported in our three cases. The involvement of mediastinal, peritoneal, and retroperitoneal is however rare [5,8,12].
Functional imaging is considered as a helpful and useful diagnostic method for the evaluation of Kikuchi-Fujimoto disease. However, its application in the diagnosis of KFD has rarely been reported due to the fewer number of patients with the diseases reported from seven previous studies (Table 3).
We reviewed 13 cases from previous eight studies and 3 cases from our study (Tables 2 and 3) [12-18]. From these 16 cases it was reported that 15 out of 16 cervical lymph nodes (bilateral in 8 patients, and unilateral in 8 patients), 7 out of 16 axillary lymph nodes (bilateral in 5 patients, and unilateral in 2 patients), 6 of 16 mediastinal lymph nodes, and 2 of 16 inguinal lymph nodes exhibited increased FDG uptake, while 4 of the 16 patients had matted extra-peritoneal lymph nodes. One study reported that the affected lymph node tend to be located in unilateral cervical region [5], however, in our study, there was no obvious preponderance in terms of nodal location. Furthermore, the study reported the estimated diameter of the affected lymph nodes was less than 35 mm, with no or mild lymph node fusion, and rarely extranodal infiltration.
The SUVmax values in the affected lymph nodes was reported to range from 4.85 to 21.1 (mean ± SD, 10.53 ± 3.02) and the mean of SUVmax values ranged from 3.5 to 17.3 (mean ± SD, 7.35 ± 4.13), while 12 out of 16 large nodes with the maximum values of SUVmax were located in the cervical region. We observed that the size (the maximum diameter and the orthogonal diameter) of the affected lymph nodes were not correlated with SUVmax in four cases. Seven patients in the seven studies had splenomegaly, but FDG uptake was rarely evident.
The negative laboratory results can help to exclude some common infectious and immunological disorders, such as tuberculosis and Systemic Lupus Erythematosus (SLE). Traditionally, CT and MRI imaging modalities have been useful in the diagnosis and follow-up of patients with KFD, particularly those with cervical lymphadenopathy. Of the two, CT scan is the most practical tool for follow-up. A patient was regarded as having KFD if he/she had the following findings,
• The affected lymph nodes were commonly located in the bilateral and unilateral cervical, axillary or mediastinal regions.
• The size of affected lymph node (the maximum diameter of enlarged lymph node not exceeding 35 mm and with no or mildmatted phenomenon).
• Mild-to-moderate FDG-avid lymph node.
• With splenomegaly which demonstrates low or no FDG uptake. However, whole body PET/CT has not been a specific diagnostic tool for KFD.
The international gold standard for the diagnosis of KFD is biopsy of the affected lymph node. We observed large number of irregular eosinophilic necrotic plaque associated with a variety of nuclear debris in the cortex or paracortex by histopathological examination. Absence of granulocytes is the most important feature of KFD.
In the management of patients presenting with fever of unknown origin and enlarged lymph nodes, it is important to consider the presence of lymphoma, tuberculous lymphadenitis, and/or malignant processes with nodal metastasis. PET/CT can offer some additional information to distinguish KFD from metastasis and lymphoma. However, it is difficult to distinguish KFD from other diseases using only the PET/CT.
One patient in our study, for example, was found to have an FDGavid node in the right cervical region and matted FDG-avid nodes in the extra-peritoneal, hepatic and hilar regions and a small FDG-avid focus in the right lobe of the liver (SUVmax 5.7). The patient also had splenomegaly which demonstrated mild FDG uptake on whole body PET/CT (Figure 2). This patient was initially highly suspected of having lymphoma but later the final diagnosis of KFD was confirmed by biopsy of the affected cervical lymph node. For a patient with lymphoma, the affected lymph nodes commonly occur in the cervical regions and a chain of matted enlarged lymph nodes which look like a mediastinal mass. The mediastinal mass is FDG-avid and in patient with lymphoma, it is commonly observed in Hodgkins Disease, while nodal and extra-nodal involvement (seen in almost all organs, such as liver, spleen, spinal and so on) is commonly observed in Non- Hodgkins Lymphomas with FDG-avid.
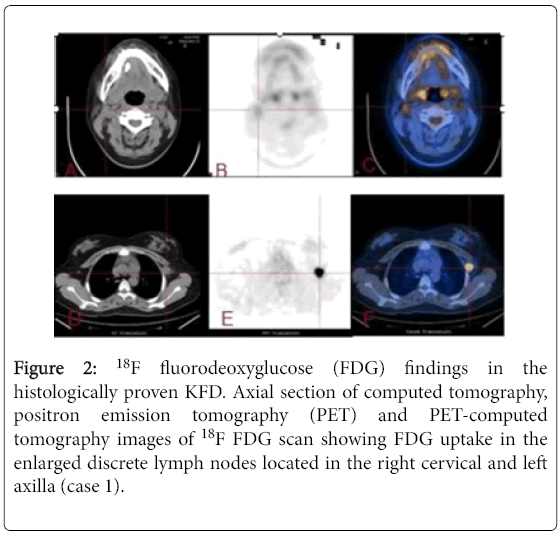
Figure 2: 18F fluorodeoxyglucose (FDG) findings in the histologically proven KFD. Axial section of computed tomography, positron emission tomography (PET) and PET-computed tomography images of 18F FDG scan showing FDG uptake in the enlarged discrete lymph nodes located in the right cervical and left axilla (case 1).
The affected lymph nodes in this case are usually larger and more matted on PET/CT (Figure 3). Previous authors had reported the maximum standardized uptake value (SUVmax) in KFD patients was not different from that in patients with lymphoma [18]. On the other hand, in a patient with tuberculosis who presents with fever, enlarged lymph nodes and other constitutional symptoms, it is the results from other TB investigations that can help to establish the diagnosis of TB while PET/CT will only detect other TB focus and FDG-avid foci in other organs and no splenomegaly.
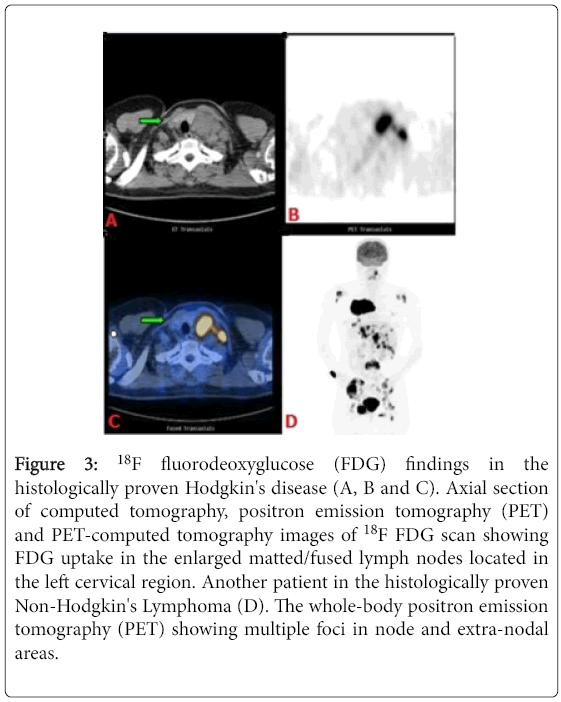
Figure 3: 18F fluorodeoxyglucose (FDG) findings in the histologically proven Hodgkin's disease (A, B and C). Axial section of computed tomography, positron emission tomography (PET) and PET-computed tomography images of 18F FDG scan showing FDG uptake in the enlarged matted/fused lymph nodes located in the left cervical region. Another patient in the histologically proven Non-Hodgkin's Lymphoma (D). The whole-body positron emission tomography (PET) showing multiple foci in node and extra-nodal areas.
For a patient with metastastic lymph nodes, it is difficult to distinguish the primary from secondary malignant cells if the original focus is not clear on PET/CT, although the metastasis may be evident in some extra-nodal areas during whole body PET/CT scan. For this type of patient who usually has poor physical and immunological status, tumor markers can help to detect presence of malignancy. The final diagnosis, however, will be determined by biopsy of the affected lymph nodes.
Although reported cases and literature on the application of PET/CT for the diagnosis of KFD is very limited, PET/CT scan may be a very useful tool that can offer some additional information than conventional imaging modalities to distinguish KFD from metastasis, TB or malignant lymphoma and therefore save the patients from invasive diagnostic procedures and unnecessary costs of prolonged treatment.