Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2017) Volume 6, Issue 4
Introduction: Primary hyperparathyroidism (PHP) is a curable disease because most patients have only one adenoma and can fully recover after adenoma removal at the location determined by preoperative imaging. However, many Japanese surgeons believe that intraoperative intact PTH measurement (IOPM) is essential to the surgery. Hence, many general surgeons in Japan are unable to perform surgeries for PHP in their local hospitals and must refer the patients to urban high volume centers that have introduced IOPM, even though they are experienced in general surgery and the surgery for PHP is technically simple and related to general surgery. So, we analyzed the relationship of surgical outcomes, with and without IOPM.
Method: Between January 2007 and December 2016, 183 consecutive patients with PHP underwent surgery in our institution. We performed the surgery between 2007 and 2012 without IOPM, and starting from 2013 we performed the surgery with IOPM. We compared and evaluated the cure rate and surgical complications between patients who underwent unilateral neck exploration without IOPM with clear preoperative localization of the affected adenoma, and those who underwent any surgery with IOPM.
Result: There was no significant difference in cure rate between the two groups and there were no surgical complication in either group.
Conclusion: In cases where preoperative imaging is able to clearly localize the affected adenoma and an experienced general or endocrine surgeon performs the surgery, there is no significant difference in overall cure rate and surgical complications with or without IOPM. Though many hospitals in Japan currently do not perform IOPM routinely, our study may encourage many general surgeons to perform the surgery without IOPM.
<Keywords: Primary Hyperparathyroidism; Parathyroid hormone; Parathyroidectomy; Localization; Imaging system
Primary Hyperparathyroidism (PHP) is a curable disease because most patients have only one affected adenoma and can recover after adenoma removal at the location determined by preoperative imaging. However, some patients have multiple parathyroid glands that have adenomas or have abnormal glands, and in such cases, it is more crucial that the precise localization of the affected parathyroid glands is determined before the surgery by using a preoperative imaging system, such as Technetium-99m(Tc-99m) sestamibi scans, ultrasound examination (US), CT scans or PET-CT. There are many reports showing that accurate preoperative localization of the parathyroid affected by the adenoma is important and essential in order for focused parathyroidectomy to be performed safely, and we are in agreement. Furthermore, many surgeons believe intraoperative intact parathyroid hormone (iPTH) measurement is even more important and essential to successful and safe parathyroidectomy. However, in Japan, many hospitals currently have not introduced intraoperative iPTH measurement (IOPM) as a routine and the use of IOPM is still limited. The reason for this is that the cost of introducing the system is too high to justify its cost in the hospital when the rarity of surgery for the disease is considered. Therefore, many general surgeons in Japan are unable to perform surgeries for PHP in their local hospitals and must refer the patients to urban high volume centers that have introduced IOPM, even though they are experienced in general surgery and the surgery for PHP is technically simple and related to general surgery.
In Japan, considering the fact that limited hospitals can use IOPM due to the cost, it is very important to determine if surgical outcomes are worse without IOPM, and which type of surgery is better suited in the absence of IOPM.
In this study, we gathered clinical data on all patients who underwent surgery for PHP at Fujita Health University Hospital, Toyoake, Aichi, Japan, between January 2007 and December 2016, where the surgery was performed by one of the authors. We all belong to the Department of Endocrine Surgery in Fujita Health University, and we are sufficiently experienced in general and endocrine surgery. Between January 2007 and December 2016, 183 consecutive patients with PHP underwent surgery in our institution. Our institution is considered a high volume center in Japan, however, IOPM was not introduced until 2013 due to the cost, and 102 patients underwent the surgery without IOPM between 2007 and 2012, while 81 patients underwent the surgery with IOPM from 2013 onwards.
We recorded preoperative imaging of at least two imaging modalities (including US and sestamibi scan), preoperative and postoperative laboratory data including preoperative serum calcium levels, iPTH levels, medical examination by interview including clinical history, previous history, physical findings and postoperative physical findings including condition of vocal cords and symptom of hypoparathyroidism (tetanic syndrome). We also recorded intraoperative findings including rapid iPTH levels, condition of the recurrent nerve, and condition of the thyroid and surrounding tissues. After 2013, a blood sample for baseline iPTH level measurement was drawn before any significant dissection or retraction was performed. If a clinically affected adenoma was identified and resected and subsequently accompanied by a greater than 50% drop or a drop to within normal range in rapid iPTH level in a second blood sample 15 minutes later, additional surgical exploration was abandoned. If no drop in iPTH level was detected, further surgical exploration was performed until a greater than 50% drop or a drop to within normal range in iPTH level was identified definitively. Failure to identify an adenoma led to further surgical exploration on the side of the missing parathyroid gland, which comprised unilateral cervical further exploration. When this exploration failed to identify the missing adenoma, a similar exploration of the opposite side (bilateral neck exploration) was carried out. We adopted and performed surgeries based on the above criteria and procedure and the recurrent nerve was preserved in all cases.
Of the 183 patients, patients were divided into three groups, where one group underwent unilateral neck surgical exploration without IOPM and was judged to have clear preoperative localization of the affected parathyroid gland (between 2007 and 2012, Group 1, n=80), one group underwent any surgery (focused or unilateral or bilateral neck exploration) with IOPM (after 2013, Group 2, n=76), and others including all patients with renal failure, hereditary disorder, and patients who had recurrent disease in this study (from 2007 to 2016, Group 3, n=27) (Figure 1). In order to analyze the relationship of surgical outcomes between the patients with clear preoperative localization undergoing surgery without IOPM, and the patients undergoing surgery with IOPM, we compared and evaluated the cure rate and complications between Groups 1 and 2.
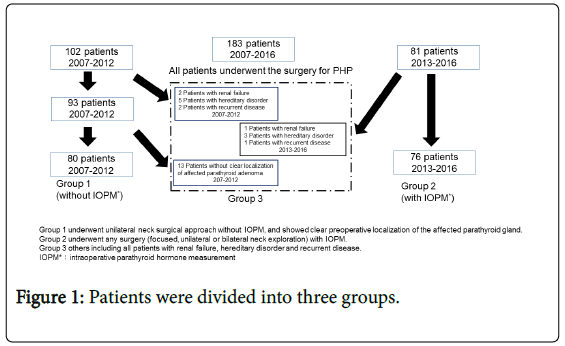
Figure 1: Patients were divided into three groups.
The sample size was estimated based on the principle of detecting a 5% difference in the incidence with a 90% probability at P<0.05. Statistical analysis of categorical variables was performed using χ2 test and that of continuous variables was performed using the Student’s t test by commercially available software (SPSS).
There was no significant difference between groups 1 and 2 in age, gender, preoperative Ca level, and preoperative PTH level (Table 1), and there was no significant difference in the cure rate between groups 1 and 2 (Table 2). Furthermore, there was no surgical complication (including recurrent nerve injury, permanent parathyroid dysfunction and postoperative bleeding) in both groups (Table 2).
| Categories | Group 1 | Group 2 |
|---|---|---|
| Age: mean | 60.5 | 59.9 |
| Gender | ||
| Female (%) | 58 females (72.5%) | 51 females (67.1%) |
| Male (%) | 22 males (27.5%) | 25 males (32.9%) |
| Weight of affected parathyroid adenoma (mg): mean | 1050.4 | 1136.5 |
| Preoperative Ca level (mg/dl): mean | 11.6 | 11.4 |
| Preoperative iPTH level (pg/ml): mean | 330.2 | 341.8 |
All Categories with no significant change. X2 test for gender category and student T-test for others
Table 1: Comparison of categories in Group 1 and Group 2.
| Group 1 | Group 2 | ||
|---|---|---|---|
| Cure rate (at first surgery) | 97.5% | 100% | P Value = 0.165 |
| Surgical complications | |||
| Recurrent nerve injury | 0 | 0 | Not applicable |
| Permanent parathyroid dysfunction | 0 | 0 | Not applicable |
| Postoperative bleeding | 0 | 0 | Not applicable |
Cure rate category with no significant difference by X2 test. There is no surgical complication among Group 1 and Group 2
Table 2: Comparison of outcomes in Group 1 and 2.
Group 1
The overall cure rate of the 80 patients in this group at first surgery was 97.5%, only two patients were not cured from the disease by the first surgery (Figure 2). An enlarged parathyroid gland was found intraoperatively on the same side (including the same site) as indicated by the preoperative imaging study in 79 of the patients (98.5%) in Group 1, so we determine that unilateral neck exploration was performed correctly and they were cured from the disease (Figure 2). Though one of the 79 patients underwent unilateral exploration at the same side as indicated by the preoperative imaging study, he was not cured from the disease even though there was only one adenoma and was present on the same side as indicated by the preoperative imaging study and explored on the first surgery. The patient underwent a postoperative localization study and reoperation, and was finally cured, and we reflected that we did not explore sufficiently after resection of a slightly swollen parathyroid gland that was localized clearly by preoperative imaging. In contrast, one patient with unilateral neck exploration was not cured and was followed for the elderly and had persistent disease. We speculate that he had another affected adenomas, in addition to a resected parathyroid adenoma on the same side as indicated by the preoperative imaging study.
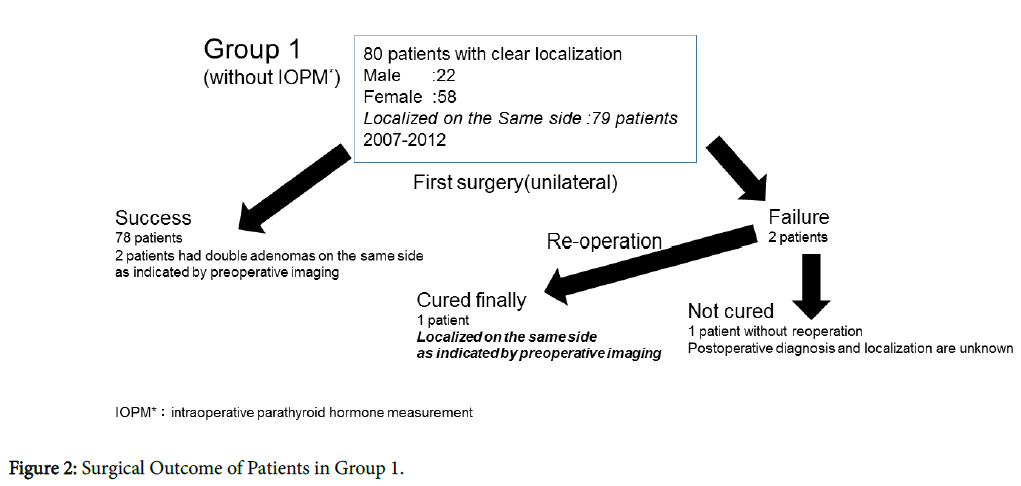
Figure 2: Surgical Outcome of Patients in Group 1.
No patient had any complications including recurrent laryngeal nerve injury, permanent parathyroid dysfunction and postoperative bleeding (Table 2).
Group 2
The overall cure rate of the 76 patients in this group at first surgery was 100%. No patient had persistent disease. A drop of 50% or more in intraoperative PTH level compared to the preoperative level was observed at 15 minutes after removal of enlarged parathyroid gland was observed in 72 patients (94.7%), the remaining four patients underwent further surgical exploration and they were all cured, where three patients had another affected adenomas, (one patient on the same side and two patients on the opposite localized by preoperative imaging). Though the intraoperative PTH level of one patient failed to drop by 50% or more compared to the preoperative level, he had more than a 50% drop after about 60 minutes (the patient underwent further surgical exploration but no gland was resected). We do not know the cause for the delay of the drop, and speculate that there could have been an error in the measurement procedure. All enlarged parathyroid glands were found intraoperatively on the same side as indicated by the preoperative imaging study in 74 of the patients (97.4%) in Group 2. Though 73 patients underwent unilateral exploration and the remaining three patients underwent bilateral exploration in Group 2 (Figure 3), no patient had any complications including recurrent laryngeal nerve injury, permanent parathyroid dysfunction and postoperative bleeding (Table 2).
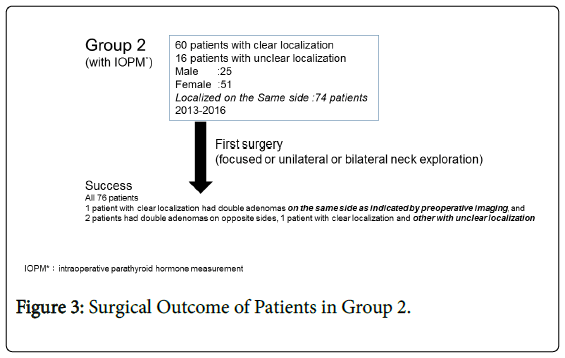
Figure 3: Surgical Outcome of Patients in Group 2.
Patients with clear localization of affected adenomas by preoperative imaging have been cured of their disease after undergoing an appropriate surgical procedure, as almost all the patients with PHP had affected adenomas on the side indicated by preoperative imaging. With the wide use of sensitive preoperative localization studies, some veteran general surgeons have advocated the use of a unilateral approach [1-3], or even minimally invasive [4], or image-guided parathyroid surgery [5,6], and the potential benefits of these procedures are decreased risks of postoperative hypocalcemia and recurrent nerve injury, and a shorter operating time [7-9]. Therefore, can IOPM rule out the patients with multiple adenomas and make the surgery more successful and safer? After the intraoperative iPTH assay was introduced by Nussbaum et al. in 1988 as a tool to assist surgeons during parathyroid surgery [10], several reports have confirmed its validity in determining whether all hyperfunctioning parathyroid glands have been removed, but there is no consensus on its routine use [11-15].
In contrast, because most patients have a single adenoma, focused or unilateral parathyroidectomy without IOPM has been reported to result in an excellent surgical outcome [16-19]. We have to take these two opinions and the demand on patients to undergo the surgery in their local hospitals in absence of IOPM into consideration carefully.
So we believe that if the surgery for PHP is safe and effective without IOPM, the surgery should be performed in the local hospital without IOPM. This removes the need for patients with PHP to go to a distant urban hospital and also reduces their economic burden. The main aim in this study was to confirm the safety and efficacy of the surgery for PHP without IOPM by selection of patients.
In our retrospective study, in patients (without renal failure, hereditary disorder, or recurrent disease) with clear preoperative localization of the affected adenoma, the cure rate was 95.7% by focused neck exploration and 98.6% by unilateral exploration, thus in unilateral neck exploration, IOPM was useful in only one patient in Group 1 and one patient in Group 2. Moreover, there was no significant difference between Group 1 (without IOPM) and Group 2 (with IOPM) in overall cure rate and surgical complications.
The result of this study shows that the surgery can be confidently performed without IOPM, when the patient has a clear preoperative image of the affected adenoma, and the experienced general or endocrine surgeon should perform unilateral neck exploration enough. In addition, our study showed there was no significant surgical complication in enough unilateral neck exploration without IOPM (Table 2), and we are confident that without IOPM, unilateral neck exploration would be more desirable than minimally invasive surgery to avoid reoperation.
Until now, many general surgeons in Japan must give up the surgery of PHP in their local hospitals and must introduce the patients to urban high volume centers with IOPM, we deeply concerned about the fact and economic and physical burden of patients with PHP.
Certainly, we could not conclude the surgery without IOPM was better than with IOPM, but we believe that we could have concluded the surgery without IOPM was equal to with IOPM after selecting patients properly, thus we expect the paper will encourage experienced general surgeons in the local hospitals in Japan to perform the surgery and relieve economic and physical burden of patients with PHP hoping to undergo the surgery in their local hospitals.
In conclusion, for veteran general and endocrine surgeons, the surgery for PHP is relatively easy and safe, and taking the improvement of imaging into consideration, we feel that IOPM can be omitted with a clear preoperative image and correct unilateral neck exploration.
Given the current state of limited hospitals with IOPM, it may be necessary to limit the use of IOPM to patients who would benefit from it significantly.
Our study shows that patients with clear preoperative localization of the affected adenoma and correct unilateral neck exploration benefit little from IOPTH, while benefiting patients that fail to localize the affected adenoma preoperatively. These patients with unclear preoperative localization perhaps should be referred to high volume centers.