Medicinal & Aromatic Plants
Open Access
ISSN: 2167-0412
ISSN: 2167-0412
Research Article - (2016) Volume 5, Issue 5
Background: The antihypertensive effectiveness of extracts from Hibiscus sabdariffa, has been reported in clinical studies of short term. This paper reports the therapeutic effectiveness, safety, and tolerability of an Herbal medicinal Product of Hibiscus sabdariffa administered during 16 weeks to hypertensive patients.
Study design: Randomized, double-blind, controlled clinical trial. Patients: Adults with mild-to-moderate hypertension. Interventions: Experimental, capsules with H. sabdariffa extract (standardized in 100 mg of total anthocyanins); Control, capsules with Lisinopril (5 mg). Dosage: One capsule every 12 h for 16 weeks. Primary outcome: Therapeutic effectiveness (reduction ≥ 10 mmHg of baseline diastolic blood pressure); Tolerability (absence of intense adverse reactions); Safety (absence of pathological changes in liver and kidney biochemical tests).
Statistical analyses: χ2, Student t, log-rank tests and ANOVA for repeated measurements.
Results: One hundred fifteen subjects were included; 57 comprised the experimental group. The therapeutic effectiveness observed in the control group was greater than that in the experimental group (p=0.0001); however, the experimental group showed a significant reduction of the blood pressure at the end of 16 weeks of treatment (24/14 mmHg; p=0.0001). Fourteen patients did not tolerate the nocturnal dosage of experimental treatment (24.5%), reporting increase in nocturnal urinary frequency, and a sole control patient did not tolerate the treatment (1.7%; p=0.0003). Safety was 100% with both treatments.
Conclusions: In hypertensive subjects, the therapeutic effectiveness of herbal medicinal product of H. sabdariffa (200 mg of anthocyanins/daily), administered during 16 weeks, was less than that of Lisinopril; however, the experimental treatment significantly reduced systolic and diastolic blood pressure and shows 100% safety. Because H. sabdariffa extract acts as diuretic, the night administration is contraindicated. More clinical studies are necessary to better evaluate the effectiveness and tolerability of the chronic administration of H. sabdariffa standardized extracts in hypertensive patients.
Keywords: Malvaceae; Hibiscus sabdariffa; Anthocyanins; Herbal medicinal product; Arterial hypertension; Controlled and randomized clinical trial
ACE: Angiotensin-Converting Enzyme; AC: Anthocyanins; ALT: Alanine Aminotransferase; AST: Aspartate Aminotransferase; BMI: Body Mass Index; BP: Blood Pressure; DBP: Diastolic Blood Pressure; HDL: High Density Lipids; HMPHs: Herbal Medicinal Product of Hibiscus sabdariffa; IMSS: Mexican Institute of Social Security; IMSS-GH-C: IMSS General Hospital in Cuernavaca, Morelos, Mexico; ITT: Intention-To-Treat; JNC VII: Joint National Committee VII; LDL: Low Density Lipids; NCEP-ATP III: National Cholesterol Education Program-Adult Treatment Panel III; NOM-030-SSA2-2009: Official Mexican Norm for the Prevention, Treatment and Control of Arterial Hypertension; PDA: Photodiode Array; SBP: Systolic Blood Pressure; TAC: Total Anthocyanins; TFA: Trifluoroacetic Acid.
Hibiscus sabdariffa L. (Malvaceae) is a plant species employed in many cultures worldwide with culinary and therapeutic purposes, including its antihypertensive effect [1,2]. In diverse preclinical investigation models, the aqueous extract containing the dry calyxes of H. sabdariffa has showed antihypertensive activity, which is exercised through various synergic mechanisms of action, mainly as an ACE inhibitor [3-5], as a diuretic [6-8], as a calcium channel antagonist [9,10], and as a modulator of nitric oxide activity [8,9,11]. It was recently demonstrated that the polyphenol-rich extract of H. sabdariffa reduces angiotensin II (AT1) peripheral receptors, and that the diuretic effect of the H. sabdariffa aqueous extract is exercised mainly by modulating aldosterone activity [12,13]. Additionally, phytochemical studies have identified the group of the major compounds present in the aqueous extract, that is anthocyanins, which are denominated delphinidin-3- O-sambubioside, and cyanidin-3-O-sambubioside (Figure 1) [3,14]. The antihypertensive activity, exerted as ACE inhibitors, is attributed principally to these latter two compounds [5]. Some clinical studies coincide in that H. sabdariffa extracts, administered for periods of 2 to 6 weeks, diminishing SBP by between 7 and 21 mm Hg, and DBP by between 11.46 and 13.1 mm Hg. The majority of these studies have utilized infusions prepared with H. sabdariffa dry calyxes, but without standardizing these in terms of the content of some active principle [6]. On the other hand, there are few publications that corroborate the antihypertensive effect of H. sabdariffa standardized extracts in patients with hypertension. A sole clinical assay has employed an Herbal Medicinal Product of H. sabdariffa (HMPHs), standardized in 250 mg of Total Anthocyanins (TAC), administered during 4 weeks, in which BP was reduced from 146/98 to 130/86 mmHg [4]. In addition, in previous clinical studies, side effects have not been reported with the administration of H. sabdariffa extracts, nor have there been alterations in hepatic and renal function tests [6,15-20].
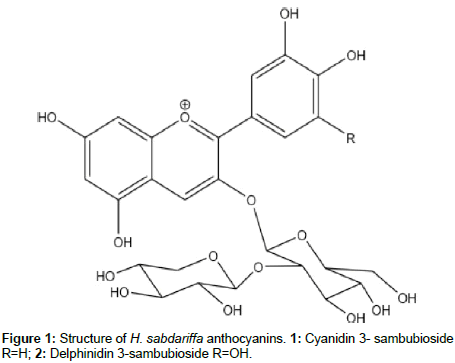
Figure 1: Structure of H. sabdariffa anthocyanins. 1: Cyanidin-3-O-sambubiosideR= H; 2: Delphinidin-3-O-sambubioside R=OH.
Despite previous reports, there are, to our knowledge, no studies of the hypertensive effect of the H. sabdariffa standardized extract administered for longer periods. The objective of the present clinical study was to evaluate the therapeutic effectiveness of a novel HMPHs elaborated with an organic extract and standardized in TAC, administered during 16 weeks to hypertensive patients.
Plant material
For the experimental treatment, H. sabdariffa calyxes were obtained from a controlled crop developed in Xochitepec, Morelos State, Mexico (December 2010). Abigail Aguilar, MSc, identified the vegetal material and a voucher was deposited in the IMSS herbarium (Ref. 14290).
Extraction and treatments formulation
The plant material (50 kg) was dried under conditions of darkness at room temperature. An electric mill was utilized to obtain ground particles of <6 mm. Dry calyxes (15 kg) were macerated during 48 h with a 64:30:6 ethanol/acetone/water solution with a 1:8 mass/volume proportion (2 times). Afterward, the extract was evaporated under reduced pressure to 25% of the total volume. To this extract were added ascorbic acid at concentration of 500 mg/mL and beta- cyclodextrin (Kleptose®; France) at a concentration of 800 mg/mL. This mixture was finally freeze-dried to obtain a homogeneous powder, which was stored until its use in the phytopharmaceutical formulation. Each capsule of experimental treatment contained an average of 100 mg of TAC. After quality-control tests, the product was packed in single-dose, hermetic, aluminum pill envelops. For the control treatment, Lisinopril (USP 5 mg/capsule) was mixed with artificial flavoring and coloring and then reunited with the appropriate pharmaceutical vehicle and packed in identical pill envelopes.
Calibration curves
Experiments were carried out in a Waters 2695 separations module system equipped with a Waters 996 PDA detector (Waters Corp., Milford, MA, USA), and was utilized empower chromatography manager ver. 1 software (Waters Corp.). Analysis was developed with a Merck Lichrosphere RP-18 column (5 μm 250/4.0 mm). The mobile phase consisted of 1.1% (v/v) of aqueous TFA (solvent A) and acetonitrile (solvent B). An isocratic system comprised 15% B and 85% A during 12 min. PDA, 230-600 nm: detection wavelength, 520 nm. Flow rate was maintained at 1 mL/min, column temperature was 30°C, and injection volume was 20 μL. Previously isolated AC 1 (4 mg) and 2 (4 mg) were separately dissolved in 0.1% TFA/methanol solution (v/v) (5 mL) and utilized as standard stock solutions for generating calibration curves. Concentrations of 250, 500, 1,000 and 2,000 μg/ mL were prepared for each AC, respectively. These four standard solutions were injected (20 μL) to generate a calibration curve for the two standard compounds separately. Standard curves were linear, with R2=0.9966 for AC 1 and with R2=0.9836 for AC 2 [4]. The anthocyanins delphinidin-3-O-sambubioside 1, and cyanidin-3-O- sambubioside 2, displayed retention times of 8.1 min and 8.4 min, respectively (Figure 2).
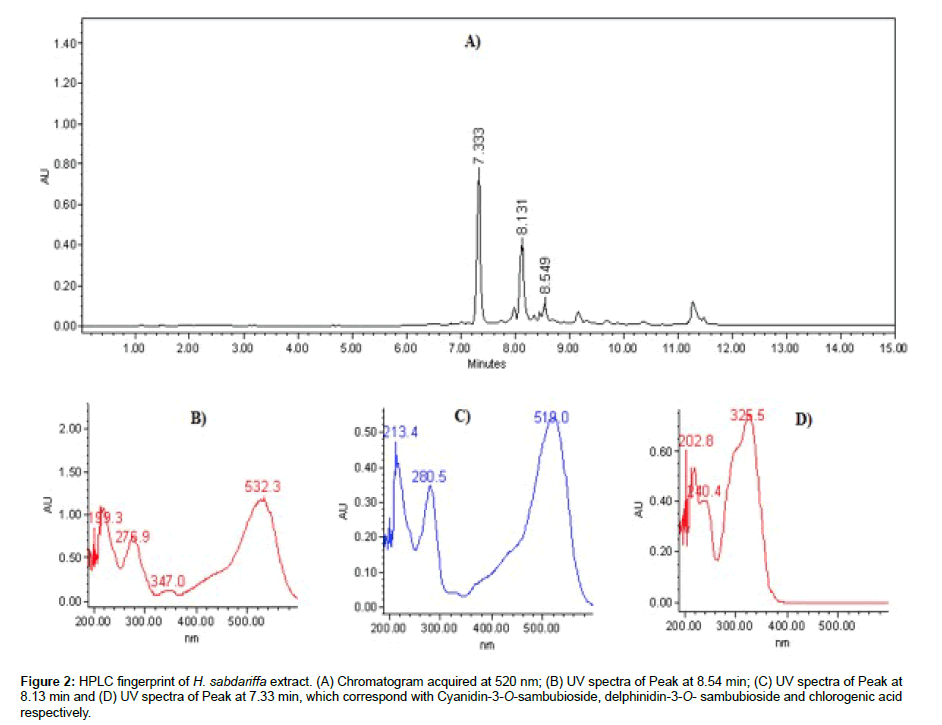
Figure 2: HPLC fingerprint of H. sabdariffa extract. (A) Chromatogram acquired at 520 nm; (B) UV spectra of Peak at 8.54 min; (C) UV spectra of Peak at 8.13 min and (D) UV spectra of Peak at 7.33 min, which correspond with Cyanidin-3-O-sambubioside, Delphinidin-3-O- sambubioside and chlorogenic acid respectively.
Study design
The study design was, in parallel groups, a randomized, doubleblind clinical study controlled with Lisinopril. Random balancedblock technique, based on a random numbers table, was utilized; and a sequential list of codes was designed in blocks of two. To the pair numbers was assigned the sequence of treatment 1-2; and to the nonpair numbers, the 2-1 sequence. To ensure blinding in drug packaging, only the code number was registered. The code list with the name of each assigned treatment remained blinded until after statistical analysis. Blinding was verified, through interrogation, at each patient’s followup visit. The HMPHs was developed at the IMSS South Biomedical Research Center in Xochitepec, Morelos, Mexico. The clinical study protocol was reviewed and authorized by the Local Investigation and Ethics Committee of the IMSS-GH-C (August 8th, 2008; Registry number R-2008-1701-28), and the assay was developed according to Declaration of Helsinki guidelines.
Subjects
These included ambulatory men and women from the IMSS-GH-C, with primary arterial hypertension at stages I (140-159/90-99 mmHg) or II (160-179/100-109 mmHg), in accordance to Official Mexican Norm NOM- 030-SSA2-2009 for the arterial hypertension [21]. These study subjects were aged between 20 and 65 years and were without antihypertensive pharmacological treatment during at least 1 month prior to entry into the clinical study. The diagnosis of hypertension was corroborated by means of the technique proposed by the same NOM-030-SSA2-2009. Patients who, during the essay, displayed treatment non-adherence, moderate or serious side effects, and/or therapeutic failure (absence of antihypertensive effect and/or hypertensive urgency), were excluded from the study, but not from the data analyses.
Interventions
The experimental intervention consisted of administration of the HMPHs, formulated in hard gelatin capsules, which contained 100 mg of TAC; doses: one capsule every 12 h (200 mg of TAC/daily), oral route, during 16 continuous weeks. The control treatment was capsules with 5 mg of Lisinopril USP, same posology (10 mg/daily of Lisinopril), route, and weeks of administration. An ACE inhibitor was employed for the control treatment, because both the JNC 7 and the NOM-030- SSA2-2009 propose the administration of an ACE inhibitor for the treatment of arterial hypertension at stages I and II [21,22].
Biochemical tests
In order to evaluate therapeutic safety, at the beginning and the end of the administration period, biochemical tests for hepatic and renal function (ALT, AST, urea and creatinine) were performed. Also, lipid profiles (TC, HDL, LDL, VLDL, and triglycerides) and fasting glycaemia were carried out to evaluate the antihypercholesterolemic and antihyperglycemic effects of the HMPHs. All of the tests were conducted on the same equipment and with the same laboratory reagents of the IMSS-GH-C.
Outcome variables
Primary outcome: Therapeutic effectiveness was considered when, at any point of the study period, the DBP showed a reduction of ≥ 10 mmHg from that identified in the baseline measurement.
Secondary outcomes
Tolerability: At any time of the administration period, the absence of undesirable effects catalogued as intense or severe and that were attributed to the assigned treatment; Safety: At the end of the study, the absence of pathological elevations, above the normal upper limits, of the biochemical hepatic and renal function tests; Non-adherence: The consumption of <80% of the indicated dose at any evaluation point; and Therapeutic failure: Hypertensive urgency and/or absence of antihypertensive effect.
Study description
After obtaining signed informed consent for study inclusion, patients were assigned randomly to one of the two treatment groups. After the initial evaluation, the patients were assigned one weekly appointment during the first 4 weeks, and after that, an appointment every 2 weeks, to the conclusion of the study. At each appointment, therapeutic effectiveness was measured (by assessment of SBP and DBP with previously calibrated electronic equipment), as well as tolerability, and treatment adherence by means of an empty capsule-vial count; in addition, the necessary amount of capsules for the following period was provided.
Statistical analyses
An ITT analysis was performed. A paired sample Student t test for analysis of continuous variables within the same group was employed, as well as for independent samples, to compare the means between the two treatment groups. χ2 test was utilized to compare two proportions; log-rank test to compare study dropouts, and repeated measures ANOVA for identifying differences in the main outcome variable, i.e., therapeutic effectiveness. Values of p ≤ 0.05 were employed to reject the equality hypothesis.
In contrast with our previous clinical study, in which the pharmaceutical presentation of the HMPHs was in the form of powder in order to reconstitute that packaged in hermetic aluminum envelopes, the presentation of the HMPHs evaluated in the present study was in hard gelatin capsules blister-packed. The TAC dose was 200 mg/daily, a lower dose than that administered in our previous clinical study, which was 250 mg/day [4]. One hundred fifteen patients initiated the study, 57 of these comprising the experimental group. Tables 1 and 2 compare patient study- entry conditions. It was observed that there were no significant differences in any of the variables evaluated (p ≥ 0.30), that is, the values were distributed homogeneously in the two treatment groups. In the whole group studied, on study entry, mean SBP was 145.14 (± 8.81 mmHg) and mean DBP was 90.03 (± 6.27 mmHg), while BMI was 29.23 kg/m2 (± 4.69 kg/m2). It was observed that the feminine gender predominated and that the frequency of smoking and alcoholism was low (<15%). However, one third of the population was obese (32.17%), with a BMI of >30 kg/m2. Table 3 compares the variables related with arterial hypertension. There were also no statistical differences between the two groups (p ≥ 0.10). The majority of subjects included were prevalent cases, in stage I of hypertension (90.4%), and with familial antecedents of hypertension (66%). In Table 4, it is possible to observe that on study initiation, there were, on average, elevations of glucose, total cholesterol, and triglycerides in the population studied. These increases, together with obesity- overweight (average initial BMI was 29.3 m/ kg2), contribute to the supposition that an important percentage of the population studied is in compliance with NCEP-ATP III criteria for metabolic syndrome [23]. During the 4 total treatment months, 35 participants were excludedfrom the study. Figure 3 depicts, by means of a Kaplan–Meier curve, the percentage of study dropouts during the 16 weeks of the study in both treatment groups, and Table 5 compares the reason for exclusion. The comparisons show that in the experimental group, there were more dropouts (p=0.01) and more side effects mainly due to the increase in nocturnal urinary frequency (p=0.0003), but less treatment non- adherence (p=0.05) than in the control group.
| Variable | HMPHs(n=57) | Lisinopril(n=58) | studentt | ||
|---|---|---|---|---|---|
| m | SD | m | SD | p | |
| Age(years) | 50.68 | 10.43 | 52.18 | 8.30 | 0.39 |
| Weight(k) | 75.40 | 14.13 | 73.32 | 13.90 | 0.42 |
| Eight(m) | 1.59 | 0.09 | 1.58 | 0.08 | 0.62 |
| BMI(k/m2) | 29.53 | 4.93 | 28.93 | 4.46 | 0.49 |
| SBP(mmHg) | 146.00 | 10.70 | 144.31 | 6.41 | 0.30 |
| DBP(mmHg) | 89.71 | 6.70 | 90.34 | 5.87 | 0.59 |
SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure
Table 1: Comparison of the characteristics of the treatment groups, at the beginning the study. Values are mean (m) and standard deviation (SD).
| Variable | HMPHs (n=57) | Lisinopril (n=58) | X2 | |||
|---|---|---|---|---|---|---|
| f | % | f | % | p | ||
| Sex | 0.79 | |||||
| Men | 21 | 36.8 | 20 | 34.4 | ||
| Women | 36 | 63.1 | 38 | 65.5 | ||
| Schooling | 0.40 | |||||
| Basic or < | 31 | 54.3 | 27 | 46.5 | ||
| High or > | 26 | 45.6 | 31 | 53.4 | ||
| Alcoholism | 0.66 | |||||
| Yes | 2 | 3.5 | 3 | 5.1 | ||
| Not | 55 | 96.4 | 55 | 94.8 | ||
| Smoker | 0.75 | |||||
| Yes | 8 | 14.0 | 7 | 12.0 | ||
| Not | 49 | 85.9 | 51 | 87.9 | ||
| Obesity (BMI>30) | 0.50 | |||||
| Yes | 20 | 35.0 | 17 | 29.3 | ||
| Not | 37 | 64.9 | 41 | 70.6 | ||
Table 2: Comparison of the characteristics of the treatment groups, at the beginning the study. Values are absolute frequencies (f) and relative frequencies (%).
| Variable | HMPHs (n=57) | Lisinopril (n=58) | Chi2 | ||
|---|---|---|---|---|---|
| f | % | f | % | p | |
| Hypertension | 0.77 | ||||
| Prevalent | 52 | 91.2 | 52 | 89.6 | |
| Incident | 5 | 8.7 | 6 | 10.3 | |
| Previous treatment | 0.19 | ||||
| Yes | 47 | 82.4 | 42 | 72.4 | |
| Not | 10 | 17.5 | 16 | 27.5 | |
| Hypertension stage | 0.10 | ||||
| 1 | 49 | 85.9 | 55 | 94.8 | |
| 2 | 8 | 14.0 | 3 | 5.1 | |
| Hypertension in relatives | 0.18 | ||||
| Yes | 41 | 71.9 | 35 | 60.3 | |
| Not | 16 | 28.0 | 23 | 39.6 | |
Table 3: Comparison of variables related to arterial hypertension. Values are absolute frequencies (f) and relative frequencies (%).
| Variable | HMPHs (n=57) | Lisinopril (n=58) | student t | ||
|---|---|---|---|---|---|
| m | SD | m | SD | p | |
| Urea | 26.86 | 6.64 | 26.12 | 9.14 | 0.6 |
| Creatinine | 0.75 | 0.2 | 0.77 | 0.22 | 0.6 |
| ALT (IU/L) | 27.47 | 12.46 | 23.88 | 8.07 | 0.06 |
| AST (IU/L) | 25.85 | 7.7 | 25.78 | 8.56 | 0.96 |
| Cholesterol | 202.39 | 35.45 | 196.24 | 36.3 | 0.34 |
| Triglycerides | 175.65 | 75.48 | 164.72 | 70.01 | 0.4 |
| Glucose | 100.85 | 23.01 | 101.19 | 25.84 | 0.93 |
Table 4: Comparison of biochemical variables at the beginning the study. Values are means (m) and standard deviation (SD) of (mg/dL).
| Cause | HMPHs | Lisinopril | X2 | ||
|---|---|---|---|---|---|
| f | % | f | % | p | |
| Side effects | 14 | 24.5 | 1 | 1.7 | 0.0003 |
| Non adherence | 2 | 3.5 | 8 | 13.7 | 0.05 |
| Therapeutic failure | 2 | 3.5 | 0 | 0 | 0.15 |
| Others | 6 | 10.5 | 2 | 3.4 | 0.13 |
| Total | 24 | 42.1 | 11 | 18.9 | 0.007 |
Table 5: Causes for study exclusion. Values are absolute frequencies (f) and relative frequencies (%).
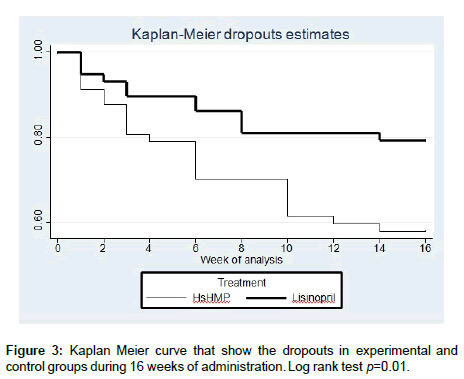
Figure 3: Kaplan Meier curve that show the dropouts in experimental and control groups during 16 weeks of administration. Log rank test p=0.01.
HMPHs nocturnal administration did not take into account the diuretic effect of the H. sabdariffa extract [7,8,13], which caused, in some patients, side effects in terms of mainly increasing nocturnal urinary frequency and discontinuous sleep. Due to this effect collateral, the nocturnal administration of the H. sabdariffa extracts must be contraindicated.
Figure 4 compares the records for SBP and DBP obtained for the two treatments during the 16 study weeks. In the experimentaltreatment curve, it was observed that the antihypertensive activity reached the highest proportion during week 1 of administration, achieving its maximal hypertensive effect at the end of the study period. In addition, it was observed that the HMPHs reduced SBP from 145 to 120 mmHg, and DBP from 90 to 75 mmHg (p=0.0001). It is noteworthy that the HMPHs, after maintaining the BP from weeks 2-10, caused to an extra diminution, from week 10 of administration, of approximately 8 mmHg in SBP and of 4 mmHg in DBP. On the other hand, in general terms, the antihypertensive activity was greater with Lisinopril; however, at the end of week 16 of administration, the values of SBP and DBP obtained by patients who completed the administration protocol in both treatment groups did not show differences (p=0.08).
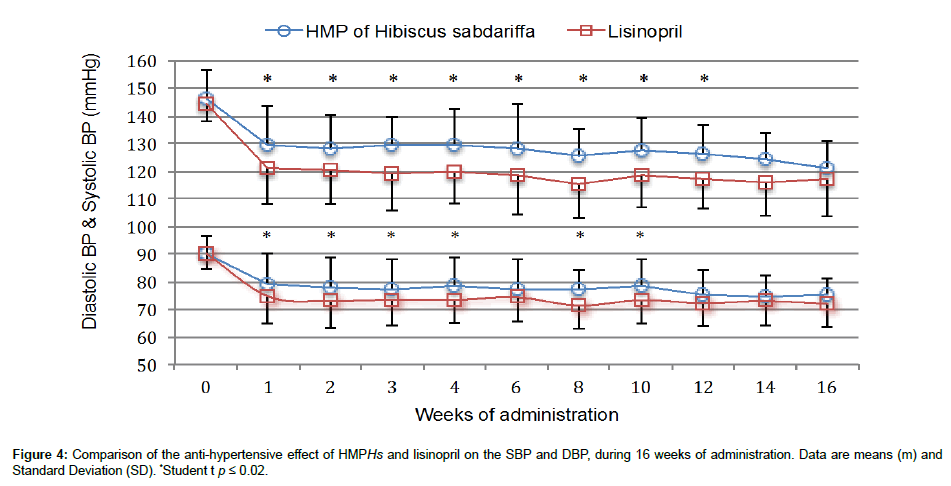
Figure 4: Comparison of the anti-hypertensive effect of HMPHs and lisinopril on the SBP and DBP, during 16 weeks of administration. Data are means (m) and Standard Deviation (SD). *Student t p ≤ 0.02.
It is noteworthy that the reduction of BP observed during the first 4 weeks of HMPHs administration in the present study (16.53/10.99 mmHg), which administered 200 mg of TAC/daily, is of a magnitude similar to that observed at the end of our previous study (16.59/11.81 mmHg), which administered 250 mg of TAC/daily in a sole morning dose during 4 continuous weeks [4]. These data confirm that the antihypertensive activity of H. sabdariffa extracts, standardized between 200-250 mg of TAC, is consistent and reproducible, although the extract employed in the HMPHs formulations would have a different polarity. Therefore, it can be hypothesized that in H. sabdariffa extracts, there are other compounds that possess antihypertensive activity, mainly polyphenols and flavonoids, with different antihypertensive mechanisms of action [8,11,13].
Figure 5 compares the percentages of therapeutic effectiveness achieved with both treatments during 16 weeks. It was observed that, in general, Lisinopril obtained greater percentages of therapeutic effectiveness, achieving significant differences at weeks 1, 8, and 10 (p ≤ 0.03); however, in the last three evaluations, the percentages of effectiveness obtained by both treatments did not demonstrate significant differences (p ≥ 0.65).
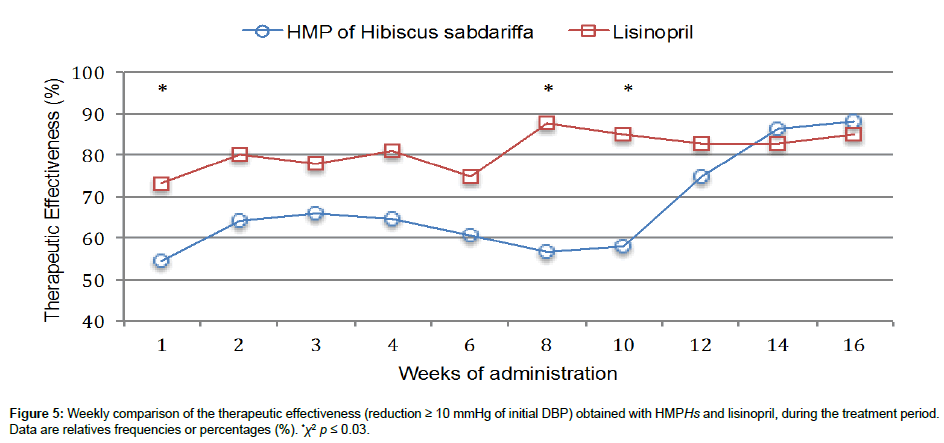
Figure 5: Weekly comparison of the therapeutic effectiveness (reduction ≥ 10 mmHg of initial DBP) obtained with HMPHs and lisinopril, during the treatment period. Data are relatives frequencies or percentages (%). *χ2 p ≤ 0.03.
To compare the means of therapeutic effectiveness obtained with each treatment, repeated measures ANOVA were performed. This was scored as No effectiveness=0, and Yes effectiveness=1. Thus, with the control treatment, 502 clinical evaluations of this variable were performed, obtaining a mean of 0.80 ± 0.01; while in the experimental group, 436 evaluations were carried out, obtaining a mean of 0.67 ± 0.02 (p=0.0001) (Figure 6). This result emphasizes that the control treatment achieved higher averages, in approximately 13%, of therapeutic effectiveness. Table 6 illustrates the effect of HMPHs on the biochemical variables. The variables that evaluated hepatic and renal function remained without modification on finalizing the study (p ≥ 0.34). These data corroborated the therapeutic safety of the extracts of H. sabdariffa, which has already been reported in different clinical studies [4,6,16-20]. Additionally, total cholesterol, triglycerides, and fasting glucose showed important and significant reductions with the HMPHs administration (p ≤ 0.02). These data are in agreement with different studies conducted in animal models and in clinical studies, which have reported the beneficial effect of the H. sabdariffa aqueous extract on dyslipidemias and hyperglycemia, as well as inhibiting effect of α-amylase, α-glucosidase and pancreatic lipase [1,2,24-28]. The effects of HMPHs on different biochemical parameters that integrate the metabolic syndrome, allow proposal of the extract as a good alternative for treating slight or moderate arterial hypertension and other alterations associated with this syndrome, a situation not shared by any other group of antihypertensive medications, including ACE inhibitors.
| Variable | Basal | Final | student t | ||
|---|---|---|---|---|---|
| m | SD | m | SD | p | |
| Urea | 26.75 | 6.55 | 26.45 | 6.73 | 0.82 |
| Creatinine | 0.74 | 0.2 | 0.77 | 0.18 | 0.37 |
| ALT (IU/L) | 26.14 | 13.32 | 24.97 | 9.92 | 0.66 |
| AST (IU/L) | 25.17 | 8.51 | 26.85 | 10.48 | 0.34 |
| Cholesterol | 207.53 | 33.15 | 189.4 | 32.2 | 0.0005 |
| Triglycerides | 171.24 | 74.9 | 153.13 | 67.91 | 0.03 |
| Glucose | 102.17 | 28.95 | 89.97 | 22.42 | 0.02 |
Table 6: Effect of the HMPHs on biochemical variables. Values are means (m) and standard deviation (SD).
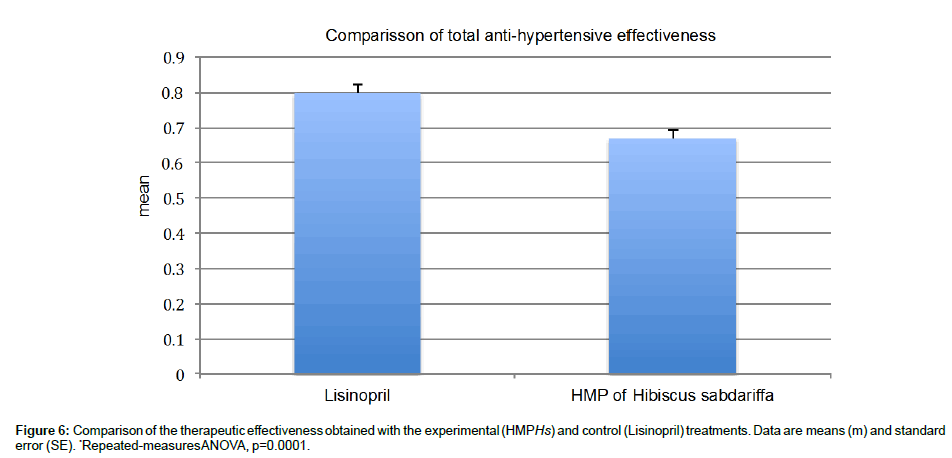
Figure 6: Comparison of the therapeutic effectiveness obtained with the experimental (HMPHs) and control (Lisinopril) treatments. Data are means (m) and standard error (SE). *Repeated-measures ANOVA, p=0.0001.
Finally, of the 33 patients who concluded the study under the experimental treatment, 29 exhibited therapeutic effectiveness (87.87%). In order to discard the confounder effect of different variables on the primary outcome, a stratified analysis was conducted. No significant differences were detected in relation to gender, obesity, smoking, alcoholism, and exercise on the therapeutic effectiveness of HMPHs (p ≤ 0.36) (Data not shown).
The HMPHs in 200 mg doses of TAC/daily (100 mg in the morning and at night), administered during 16 weeks, gave rise to important and persistent diminutions of SPB and DBP and evidenced 100% safety; however, the anti-hypertensive effectiveness of HMPHs was less than that observed with Lisinopril, but with better adherence. The HMPHs administered at bedtime caused an increase in nocturnal urinary frequency in an important percentage of subjects; thus, nocturnal schedule must be contraindicated in order to avoid this side effect, as well as to improve its tolerability, adherence, and effectiveness. On the other hand, because HMPHs also improves some biochemical parameters of patients with metabolic syndrome, it is possible for it to be considered a good alternative for the treatment of that syndrome. More clinical studies are necessary for better evaluation of the antihypertensive effectiveness and tolerability of the HMPHs employed in this essay and that of other H. sabdariffa extracts.
The present project was partially supported by CONACYT-Morelos 2008- 93473 and by PROMEP 2011 UAEMOR-PTC-260.
All of the authors manifested not having any conflicts of interest with regard to the present study.