Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2013) Volume 2, Issue 1
A 33 year old female domestic helper presented with painful thyroid swelling of several months duration which was associated with fever and recent dysphagia of about one week duration. A thyroid abscess was diagnosed by ultrasound that was subsequently drained with full coverage by appropriate antibiotics. During her laboratory work up, an elevated corrected calcium level was detected that required to be lowered transiently by a bisphosphonate (pamidronate) infusion. Fine Needle Aspiration Cytology (FNAC) of the thyroid gland and cervical lymph nodes revealed the presence of squamous cell carcinoma in the thyroid with involvement of the cervical lymph nodes. A soft and friable laryngeal growth was noted by an upper gastrointestinal endoscopy performed for assessment of her anemia. The patient condition deteriorated progressively and she died prior to completion of the full work up. The retrospective analysis of her radiological investigations wasn’t confirmatory for the presence of a primary lesion in the larynx. In conclusion, abscess in the thyroid due to primary squamous cell carcinoma is a rare and aggressive entity with poor prognosis. FNAC is effective confirmatory tool, but efforts should be made to rule out metastasis from other sites.
<Keywords: Thyroid abscess; Primary squamous cell cancer of thyroid; Secondary squamous cell cancer of thyroid
Squamous cell carcinoma (SCC) is an uncommon malignancy of the thyroid gland which can be classified according to the site of origin into a primary or a secondary. Secondary squamous cell carcinoma of the thyroid gland is usually due to either extension of SCC from adjacent structures or metastasis from a distant SCC. Primary SCC of the thyroid gland is an extremely rare neoplasm, representing less than 1% of all primary thyroid malignancies [1], and it is always crucial to look for a secondary source of malignancy prior to adoption of the diagnosis of primary SCC of the thyroid gland. In this report we present a young lady who developed an acute suppuration of the thyroid which proved to be due to SCC by FNAC. Due to the rapid clinical deterioration of the patient, a primary source couldn’t be confirmed neither could be ruled out.
A 33 year old Indian female, who is a recently appointed domestic helper, presented to the hospital on Feb 5th 2012 with progressive dysphagia and throat pain of few months duration. This has been treated as an upper respiratory tract infection by polyclinic physicians. One week prior to admission she developed painful swelling of the lower part of the neck associated with dizziness and headache. Physical examination revealed that her temperature was 38.5°C with sinus heart rate of 120 per minute and BP of 126/74 mmHg. Neck examination showed large and tender goitre with multiple nodules bilaterally. Her initial laboratory investigations are shown in table 1. The antibiotics ceftriaxone (Rocephin) and vancomycin were then initiated after taking blood cultures which turned to be positive for Streptococcus constellatus. Thyroid ultrasound showed enlarged lobulated thyroid gland which is replaced by heterogeneous masses with bilateral upper cervical lymphadenopathy (Figure 1). During follow up, the patient developed thrombocytopenia (Disseminated Intravascular Coagulation: DIC), respiratory distress with desaturation and hypotension for which she was intubated and ventilated in the Intensive Care Unit. Computed tomography (CT) of the neck and chest showed right thyroid abscess, right jugular vein thrombosis and bilateral lung consolidates (Figure 2). Adult respiratory distress syndrome (ARDS) couldn’t be ruled out with these findings. The patient then received several doses of Intravenous Immunoglobulins (IVIG) and platelet transfusion for thrombocytopenia. She improved hemodynamically and then was weaned off ventilation. FNAC followed by incision and drainage of the abscess have been performed on Feb 15th 2012. Since the patient remained without any limb movements, a brain CT was done on Feb 24th 2012 which showed left frontal intracerebral hemorrhage of 5.1×3×1.9 cm size with midline shift and mass effect. After she was seen by the neurologist and neurosurgeon, no neurological interventions were recommended due to low platelets (and DIC) and conservative care was suggested. On March 23rd, her serum calcium started to raise up to the level of 2.8 mmol/L (ref range, 2.2-2.6 mmol/L) and plateaued at the level of 2.96 mmol/L with serum phosphate level of 1.46 mmol/L (ref range, 0.8-1.4 mmol/L) and suppressed PTH at 0.32 pmol/L (ref range, 1.3-9.3 pmol/L). Pamidronate infusion was given (60 mg) which resulted in the reduction of serum calcium level (on April 4th 2012) with biochemistry data as shown in table 2. After 1-2 weeks, serum calcium increased back to the level of 2.8 mmol/L. Moreover, the patient showed some extent of bilateral diminished power which has been diagnosed by the neurologist as most likely to be a critical illness neuromyopathy and partially related to her intracerebral hemorrhage. During this time, results of the FNA showed clusters and sheets of malignant squamous cells (Figure 3). Smears from the left cervical lymph node showed many singly dispersed and clusters of malignant squamous cells with keratinized cytoplasm (Figure 3). So a diagnosis of squamous cell carcinoma of the thyroid with involvement of cervical lymph nodes has been given. During the patient’s work up for anemia, upper GI endoscopy was performed that detected a soft friable mass at the larynx obstructing passage of the endoscopy probe, which further questioned if this was the primary source of malignancy. The patient clinical condition has deteriorated rapidly and she died on April 18th 2012 upon failure of resuscitative procedures. Verification of the nature of the mass in the larynx could not be made as she died quickly and postmortem examination was not done.
| Parameter | Value | Normal range |
|---|---|---|
| Hb | 10.8 | 120-150 g/L |
| WBC | 13.0 | 3.9-10×109/L |
| PLT | 392 | 130-430×109/L |
| Na | 137 | 135-148 mmol/L |
| K | 4.51 | 3.5-5.3 mmol/L |
| Corrected Ca | 2.62 | 2.2-2.6 mmol/L |
| Phosphate | 1.18 | 0.8-1.4 mmol/L |
| Free T4 | 12.4 | 7.8-16 pmol/L |
| Thyroid stimulating hormone (TSH) | 2.09 | 0.27-4.2 μIU/ml |
| Alkaline Phosphatase | 219 | 26-88 U/L |
| Alanine transferase (ALT) | 37 | 10-60 IU/L |
| Gamma glutamyl transferase(δGT) | 162 | 7-64 IU/L |
| Aspartate aminotransferase (AST) | 26 | 10-42 IU/L |
| Creatinine phosphokinase (CPK) | 13 | 22-269 IU/L |
| Urea | 2 | 2.5-6.6 mmol/l |
| Creatinine | 20 | 60-120 U/L |
| Fasting glucose | 4.3 | 3.9-5.7 mmol/l |
Table 1: Initial laboratory data of the described case.
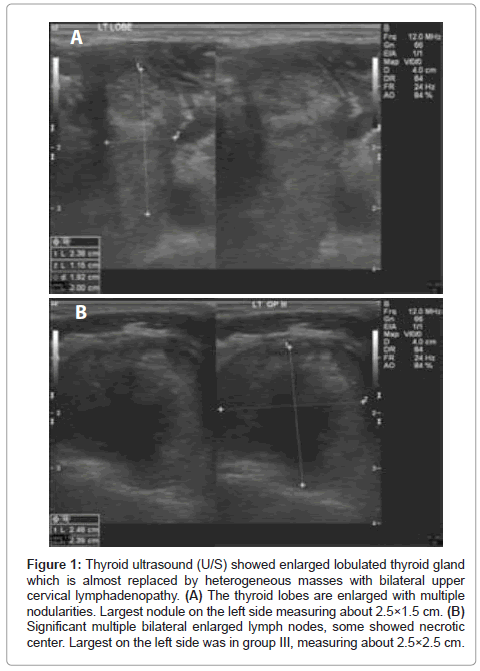
Figure 1: Thyroid ultrasound (U/S) showed enlarged lobulated thyroid gland which is almost replaced by heterogeneous masses with bilateral upper cervical lymphadenopathy. (A) The thyroid lobes are enlarged with multiple nodularities. Largest nodule on the left side measuring about 2.5×1.5 cm. (B) Significant multiple bilateral enlarged lymph nodes, some showed necrotic center. Largest on the left side was in group III, measuring about 2.5×2.5 cm.
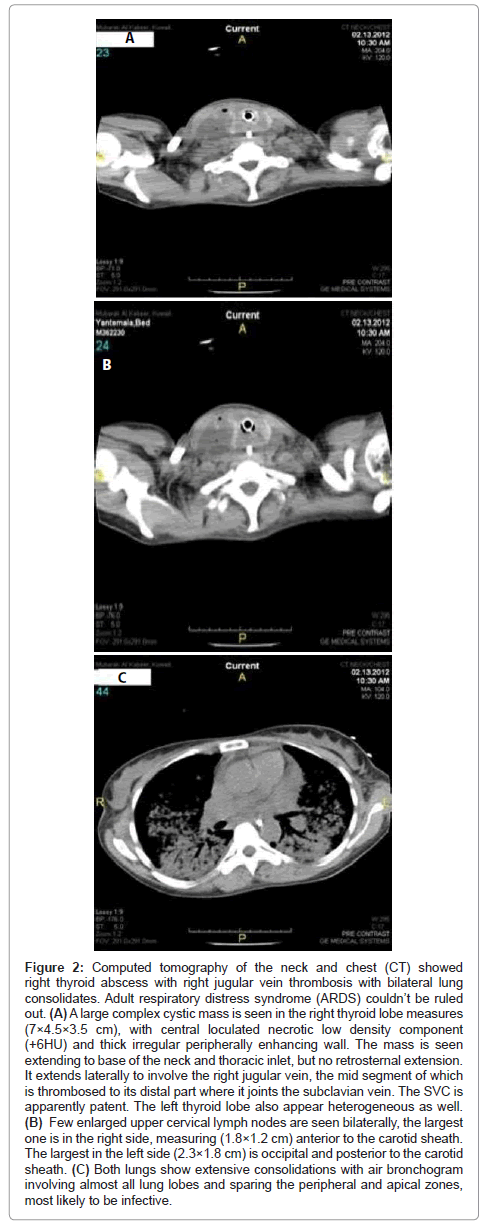
Figure 2: Computed tomography of the neck and chest (CT) showed right thyroid abscess with right jugular vein thrombosis with bilateral lung consolidates. Adult respiratory distress syndrome (ARDS) couldn’t be ruled out. (A) A large complex cystic mass is seen in the right thyroid lobe measures (7×4.5×3.5 cm), with central loculated necrotic low density component (+6HU) and thick irregular peripherally enhancing wall. The mass is seen extending to base of the neck and thoracic inlet, but no retrosternal extension. It extends laterally to involve the right jugular vein, the mid segment of which is thrombosed to its distal part where it joints the subclavian vein. The SVC is apparently patent. The left thyroid lobe also appear heterogeneous as well. (B) Few enlarged upper cervical lymph nodes are seen bilaterally, the largest one is in the right side, measuring (1.8×1.2 cm) anterior to the carotid sheath. The largest in the left side (2.3×1.8 cm) is occipital and posterior to the carotid sheath. (C) Both lungs show extensive consolidations with air bronchogram involving almost all lung lobes and sparing the peripheral and apical zones, most likely to be infective.
| Parameter | Value | Normal range |
|---|---|---|
| Corrected Ca | 2.18 | 2.2-2.6 mmol/L |
| Phosphate | 0.54 | 0.8-1.4 mmol/L |
| Alkaline phosphatase (ALP) | 594 | 26-88 IU/L |
| Alanine transferase (ALT) | 655 | 10-60 IU/L |
| Gamma glutamyl transferase (δGT) | 1028 | 7-64 IU/L |
| Aspartate aminotransferase(AST) | 509 | 10-42 IU/L |
| Creatinine phosphokinase (CPK) | 16 | 22-269 IU/L |
| Urea | 36 | 2.5-6.6 mmol/L |
| Creatinine | 45 | 71-106 μmol/L |
Table 2: Subsequent blood parameters of the case.
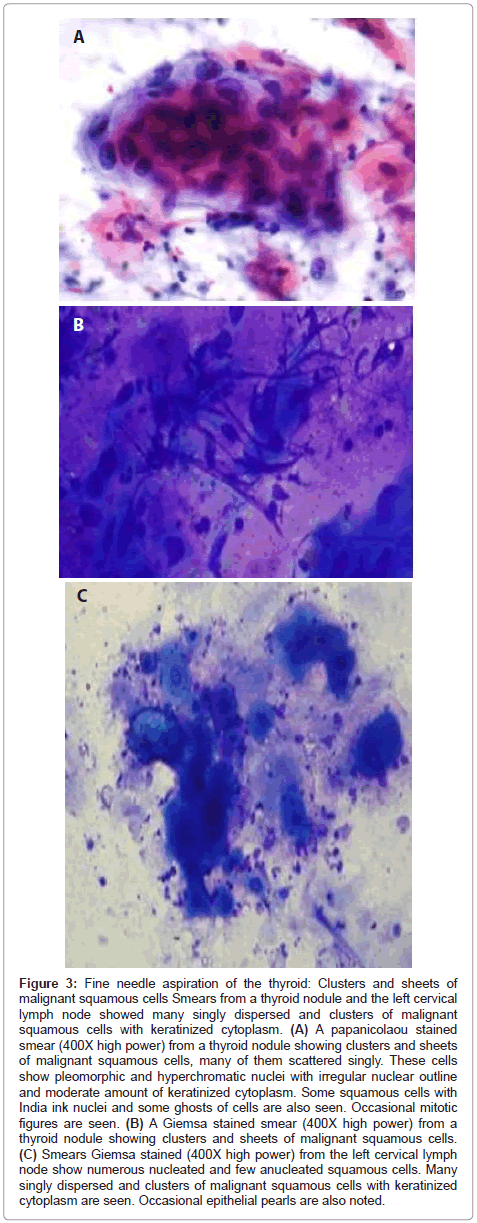
Figure 3: Fine needle aspiration of the thyroid: Clusters and sheets of malignant squamous cells Smears from a thyroid nodule and the left cervical lymph node showed many singly dispersed and clusters of malignant squamous cells with keratinized cytoplasm. (A) A papanicolaou stained smear (400X high power) from a thyroid nodule showing clusters and sheets of malignant squamous cells, many of them scattered singly. These cells show pleomorphic and hyperchromatic nuclei with irregular nuclear outline and moderate amount of keratinized cytoplasm. Some squamous cells with India ink nuclei and some ghosts of cells are also seen. Occasional mitotic figures are seen. (B) A Giemsa stained smear (400X high power) from a thyroid nodule showing clusters and sheets of malignant squamous cells. (C) Smears Giemsa stained (400X high power) from the left cervical lymph node show numerous nucleated and few anucleated squamous cells. Many singly dispersed and clusters of malignant squamous cells with keratinized cytoplasm are seen. Occasional epithelial pearls are also noted.
This unfortunate young lady has been admitted for a febrile condition associated with a thyroid swelling which proved to be acute suppuration. Her calcium level was continuously high, and this couldn’t be explained prior to the result of FNA of thyroid which showed squamous cell carcinoma with involvement of cervical lymph nodes. By definition, Primary Squamous Cell Carcinoma of the Thyroid (PSCCT) should be composed entirely of tumor cells of squamous differentiation [1]. Primary squamous cell carcinoma of the thyroid gland is a rare condition, and only relatively few cases were reported in the literature. Therefore, it is essential to rule out a secondary squamous cell carcinoma of the thyroid (SSCCT) from a primary source elsewhere prior to the designation of a diagnosis of PSCCT. According to the available work up finding of this case, the subsequent upper GI endoscopy has failed due to the presence of a soft mobile friable mass which was obstructing the nasopharynx, which raises the suspicion that the mass may be the primary source of the neoplastic process. This would be in agreement of the most likely primary sources reported in the literature which could be at the nasopharynx, lungs, tongue base, larynx, head, neck or gastrointestinal tract, and less likely at the cervix [1]. Unfortunately, a biopsy couldn’t be taken from the detected mass in our patient due to her unstable condition, the situation which rendered difficulties in the confirmation of a possible primary origin of the malignancy. Retrospective analysis of the CT films didn’t reveal any suspicious lesions in the area of larynx, neck or chest. Direct extension and metastatic involvement of the thyroid gland, despite being considered as rare by many authors, are more common than generally realized, occurring approximately 10 times more frequently than PSCC [1]. The incidence varies according to the source of the series. Autopsies on a range of tumor types usually provide an incidence rate of <5%, although this figure increases to 11-24% when multiple sections are performed [2]. There are many factors responsible for the relative frequencies of the primary site and presence of secondaries such as epidemiological prevalence, clinical behaviour, the diagnostic methods. The routine use of FNAC and various imaging modalities including FDG-PET can detect thyroid malignancies more frequently [3]. The acute presentation of our case which was due to acute suppuration had been proven by the radiological and microbiological investigations and then was treated accordingly. Too often, patients with deep neck infection due to head and neck cancer are treated by physicians who are either unaware of the possibility of head and neck cancers in this setting or who elect not to evaluate these patients because the frequency of head and neck cancers in cases of deep neck infection is believed to be extremely low. The actual incidence of head and neck cancer presenting as deep neck infection may be underestimated. The reported incidence in the literature was between 1.0% and 5.6% [4]. The clinical presentation of SCC metastases to the thyroid gland can be variable, depending largely on the extent of the primary tumor. Lam and Lo [2] studied series of patients with metastases to the thyroid; five of these cases were SCC, only one presented with an enlarging neck mass, and the rest were discovered at autopsy. In contrary, Papi et al. [5] case series included 11 cases of PSCC of thyroid, seven of which (72%) presented clinically as a rapidly enlarging thyroid nodule. About 28% of metastases to the thyroid were incidentally noted on imaging studies despite normal physical examination findings. Thyroid function test is a mandatory part in the diagnostic plan of patients suspected to have SSCCT. In Papi’s series, almost all thyroid malignancies were euthyroid at presentation and in the follow-up period, although both hypo and hyperthyroidism had been documented in such condition [6]. Tumor related hypothyroidism is caused by massive infiltration of the thyroid gland by malignant tumor; rarely, neoplastic embolization to the thyroid results in thyrotoxicosis when gland destruction occurs with leakage of stored hormones in to the peripheral blood [7]. There are no specific radiological features of secondary SCCT. Features similar to those seen in other thyroid malignancies are present. Ultrasound is usually the first radiological modality used in the diagnostic investigation of a thyroid lump. The examination is simple and costeffective, and is able to distinguish solid from cystic lesions and to define the echogenic pattern, which may suggest a benign or malignant tumors. Metastatic disease may manifest as a solitary nodule or, more commonly, as multiple nodular foci; in a patient with a known primary tumor, this should raise strong suspicion of metastatic disease. Macroscopically, metastasis to the thyroid is most often multifocal [8], unlike PSCCT, which macroscopically, might be typically restricted to one or both lobes. Ultrasound of the thyroid in our reported case revealed enlarged lobulated thyroid gland which was replaced by heterogeneous masses with bilateral upper cervical lymphadenopathy (Figure 1). Computed tomography (CT) of the neck and chest in our case showed right thyroid abscess with right jugular vein thrombosis and bilateral lung consolidates (Figure 2). Although CT is preferred, both CT and magnetic resonance imaging (MRI) scans are useful for the assessment of suspicious thyroid lumps. They allow differentiation of a thyroid mass from adjoining thyroid masses, and enable assessment of the adjacent larynx and trachea to discern displacement, luminal narrowing, vascular displacement and invasion. Evaluation should also assess calcification, cyst formation, necrosis, hemorrhage, lesion margin definition and extra-glandular extension [9]. CT of the chest, abdomen and pelvis helps to exclude a primary source for secondary SCC of the thyroid gland. In addition to CT and MRI, positron emission tomography (PET scanning) may provide useful information enabling the identification of a primary tumor in patients with occult SCC metastases to the thyroid gland [1], and this modality of investigation could be a powerful tool to delineate the source of malignancy in our case. Moreover, US guided FNAC or core biopsies are also useful diagnostic modalities when combined with clinical and radiological findings. Squamous cell carcinoma is easily recognized in cytology when features of squamous differentiation are present. PSCCT and SSCCT show the same cytological features of squamous cell carcinomas in any other organ. The aspirates tend to be very cellular, and consist of an obviously malignant population of cells with variable degree of squamous differentiation according to the tumor. The smear’s background is usually dirty, with necrosis, dyskeratotic cells, keratinized material and inflammation. The neoplastic cells may be arranged singly, in clusters, or forming syncytia. They exhibit bizarre shapes, densely hyperchromatic, enlarged nuclei, dense cytoplasm and well-defined cell borders. Cytoplasmic keratinization may be evident [10]. There has been an increase in the number of cases diagnosed and reported since the advent of routine ultrasound and FNAC of thyroid nodules. FNAC of a discrete thyroid nodule has a malignancy detection rate of approximately 80%, but the specificity for secondary malignancy is anywhere between 8 and 40%. Mijovic et al. [11] reported a high false negative rate of 13%. In fact, FNAC is the most reliable and commonly used tool to assess a thyroid mass. In our case it showed clusters and sheets of malignant squamous cells (Figure 3). Smears from the left cervical lymph node showed many singly dispersed and clusters of malignant squamous cells with keratinized cytoplasm (Figure 3). On the other hand, FNAC is unable to reliably distinguish between primary and metastatic SCC, although it is possible that immunocytochemistry may help clarify the diagnosis. Although metastatic tumors generally retain the histological features of the primary tumors, they are frequently more poorly differentiated; therefore, the definition of SCC above should be treated with caution. Because other thyroid lesions such as papillary and anaplastic carcinomas can have areas of squamous differentiation, strict criteria for the diagnosis of squamous cell carcinoma should always be applied. The association between PSCC of the thyroid and the tall cell variant of papillary cell carcinoma has been reported by several investigators [12]. Immunohistochemistry may be useful in distinguishing primary from metastatic thyroid SCC, as mentioned above. The pattern of cytokeratin expression is different in carcinomas arising from different organs, and also varies with tumor differentiation [2]. Most authors agree that while PSCC of the thyroid is positive for cytokeratin, it is negative for thyroglobulin [13]. A BRAF mutation has been reported in a PSCC case by Ko et al. [14]. So the next step in our case if we could obtain a tissue sample from the larynx mass is to utilize a single stain, or a panel of stains, specific to the known primary malignancy. Panendoscopy should be performed to exclude a primary lesion in the nasopharynx, oropharynx, hypopharynx, larynx, oesophagus and bronchus. The soft fleshy and friable mass in the larynx which could be seen upon the insertion of the endoscope is highly likely to be the source of the primary origin of the malignancy, unfortunately, this couldn’t be confirmed by having a biopsy from the mass. Given the rich vasculature of the thyroid gland, about 560 mL/100 g tissue/min, which is reported to be second only to the adrenal gland [15], it is perhaps surprising that metastasis to this site is not seen more frequently. However, observational studies have reported that metastases appear more likely in pre-existing abnormal thyroid glands. It has been hypothesized that this may be a result of the slowing of intra-parenchymal blood flow in nodular thyroid glands.
In 1931, Willis [15] proposed two hypotheses for why this is the case:
(1) Fast arterial flow through the thyroid discourages adhesion of malignant cells, and
(2) The high oxygen saturation and iodine content of the thyroid gland inhibit the growth of malignant cells. If the hypothesis of Willis is correct, diseased thyroid gland with reduced blood flow and lower iodine concentrations should be more susceptible to metastases. In 2000, Kameyama et al. reported only five cases of carcinoma metastatic to a thyroid adenoma in the literature, thus suggesting that tumor metastases are rare occurrences [16]. In 1997, Nakhjavani also noted that metastases to a pre-existing thyroid neoplasm are rare [17]. Other studies have shown that metastases to the thyroid occur more frequently in diseased gland [17]. The prognosis in our case was grave with a stormy clinical course in the hospital and very rapid deterioration in her clinical parameters which necessitated admission to the intensive care unit with partial recovery of her level of consciousness. Potentially, the patient could be managed further if she presented earlier in natural history of the ongoing malignant process. Thyroid metastasis has the same impact on prognosis as non-thyroidal metastases. Although metastases to the thyroid gland may be associated to poor prognosis, some suggest that early detection and aggressive surgical and medical treatment may improve survival in small percentage of patients. Unfortunately, Papi et al. showed that although thyroidectomy may be useful to avoid further dissemination of the primary tumor in case of solitary thyroid malignancy [5], it does not contribute to prolonging patient’s life. Likewise chemotherapy and radiotherapy, alone or in combination, did not impact on thyroid malignancy in a different manner from the nonthyroidal localizations of primary tumors, that is, there was no benefit in local disease control by palliative therapy for thyroid malignancy in the setting of the wide spread metastatic disease. Systemic chemotherapy could achieve survival gain especially in patients with metastases from the breast and colon. Interferon alpha, which is used as an immunomodulator, could affect the survival of patients with renal cell carcinoma and should be considered. In fact in the above mentioned series by Papi et al., it has been shown that the overall survival time is not significantly different in cancer patients with and without thyroid malignancy; therefore the detection of a secondary localization to the thyroid does not imply, per se, a poor prognosis. The management of SCC metastasis to the thyroid is poorly documented in the literature, primarily because the majority of the reports are derived from pathology journals that do not comment on patient’s management or prognosis. In addition, the site of the primary disease is so variable (including tongue, tonsils, larynx, oesophagus, cervix and bladder) that general comments about treatment cannot be made. Management depends on the site and the stage of the primary tumor, the presence of other metastases, and the symptoms caused by the thyroid metastases. Radical treatment for an isolated metastasis to the thyroid gland, particularly from renal cell carcinoma, can be curative, and an aggressive surgical approach has been recommended by many authors [18]. Surgery, which is almost always the initial treatment of choice, may be challenging. There is no clear consensus, but some previous studies recommended a thyroid lobectomy and/or isthmectomy in the case of a solitary thyroid metastasis and a total thyroidectomy in the case of bilateral metastases. The survival results of thyroidectomy depend on the primary tumor. A review of the evidence suggests that thyroidectomy is beneficial, even as a palliative procedure to reduce the incidence of local tumor recurrence, and can even be associated with long term survival.
For the patients with high risk for local recurrence, there are no data on post-operative radiation or irradiation in this setting, although the assumption is that the factors most predictive for recurrence will be the presence of positive margins and nodal extra-capsular extension of disease. There are data to suggest that, in addition to improving loco-regional control, full dose re-irradiation of a small volume with no elective nodal re-irradiation following surgery and in combination with chemotherapy offer potential for long-term survival. However, this strategy may also contribute to the development of late toxicity from treatment [18]. As mentioned above, delivery of optimal radiation may be hindered by nearby dose-limiting structures, in particular the oesophagus, the trachea, the laryngeal cartilages and the spinal cord. The ability to shape the X-ray beam to a precisely defined target volume allows the delivery of the optimal tumoricidal dose to the tumor bed while limiting the dose to the organs at risk. Once planning is completed, cumulative dose-volume histograms for the target volume and organs at risk enable the physician to more precisely define the risk for a given patient.
Usually patients with metastatic disease to the thyroid have poor prognosis and do not respond to conventional treatment. The survival results of all treatment modalities depend on the extent of the primary tumor, it’s response to treatment and the other co-morbidities. In our presented case, since the full workup plan couldn’t be completed, the whole clinical scenario may favour the diagnosis of secondary squamous cell carcinoma, as supported by the fact that the SSCCT is more prevalent than PSCCT and the existence of the soft friable mass in the larynx upon insertion of the endoscope. However, PSCCT can’t be ruled out especially if we consider the lack of detailed history. As stated earlier, PSCC of the thyroid gland is an extremely rare neoplasm, representing less than 1% of all primary thyroid malignancies. It frequently coexists with other mostly well differentiated thyroid carcinoma, particularly papillary thyroid carcinoma, so it’s vital to uncover the patient history carefully. Unfortunately part of the patient’s history was not explored optimally due to the language barrier as well as the fact that she was too sick and tracheostomized while she was in the intensive care unit and the general ward. Clinically, PSCC of the thyroid is very aggressive, as in our case as the time interval between the first presentation and death was reported to be 5 months; in this respect, it resembles anaplastic thyroid carcinoma [19]. Patients typically present with a rapidly increasing neck mass invading the strap muscles, soft tissues and blood vessels of the neck, compressing the trachea and oesophagus, and have accompanying cervical lymphadenopathy. Dysphagia, dyspnea, hoarseness of voice and neck pain typically ensue. It is usually a rapidly progressive malignancy with a predilection for extensive local invasion, and metastasis, which usually involves the lungs, lymph nodes, liver and mediastinum. Other rare tumors [20] that should be considered in the differential diagnosis of PSCC of the thyroid are mucoepidermoid carcinoma (MEC) and sclerosing MEC with eosinophilia. Morphologically, MEC is characterized by a mixture of squamous and mucinous component. Cytological features of thyroid MEC are identical to those seen in salivary glands, and the specific findings will depends on the grade of the tumor (low grade vs. high grade). On the other hand, sclerosing MEC with eosinophilia is characterized by the presence of squamous and glandular components in the background of marked stromal sclerosis, eosinophils and lymphoid cells. However, because this tumor is very unusual and there is not enough documentation about its cytological findings, a precise diagnosis would be very challenging in cytology. Carcinoma showing thymus-like differentiation of the thyroid (CASTLE) is another differential diagnosis. It is a very rare malignant neoplasm with about 50 cases reported in the literature, and is recognized as an independent clinicopathological entity. It is included in the World Health Organization’s classification of tumors of endocrine organs. It is morphologically similar to thymic carcinoma and may show squamoid areas or epidermoid differentiation within intercellular bridges and even focal keratinization, resembling lymphoepithelioma and SCC. However, this tumor has a characteristic immunophenotype (positive for CD5, p63, high molecular weight cytokeratin, CEA, CD117, bcl2 and galectin 3) that is hybrid between thymic carcinoma and normal solid cell nests of the thyroid and is not shared with other carcinomas such as PSCCT and SSCCT. There are no specific radiological features of PSCCT. Features similar to those seen in other thyroid malignancies are present. Ultrasound is usually the first radiological modality used in the diagnostic investigation of a thyroid lump. It has been demonstrated that distinctive ultrasound findings, for example, hypoechogenicity, ill-defined margins, intranodular vascularization and punctate calcifications (PC), accurately predict primary thyroid carcinomas. In particular, PC is considered the US counterpart of psammoma bodies peculiar to papillary and medullary thyroid carcinomas. Therefore, the evidence of PC in individuals with thyroid nodule(s) and history of nonthyroidal malignancy may help to orientate towards the diagnosis of primary thyroid neoplasm. Moreover, US guided FNAC or core biopsies are also useful diagnostic modalities when combined with clinical and radiological findings. Although CT is preferred, both CT and magnetic resonance imaging (MRI) scans are useful for the assessment of suspicious thyroid lumps. In CT, PSCC of the thyroid often tends to encase the oesophagus rather than invade it, leaving a fat plane between the tumor and the oesophagus, which is useful in confirming that the tumor arose from the thyroid rather than the oesophagus itself. It is of crucial to indicate that PSCC of the thyroid has a clinical course resembling anaplastic carcinoma and complete surgical resection is rarely possible. Unfortunately, most patients die from locally aggressive disease within 1 year [19].
This case demonstrates that a full panel of investigative procedures should be undertaken to look for primary sources of malignancy prior to diagnosing the case as PSCCT. It is vital to exclude secondary invasion of the thyroid gland from adjacent structures before making a diagnosis of primary thyroid SCC. The challenge in this case was to prove that the thyroid gland is the source of the primary malignant process after excluding metastases to the thyroid gland; this couldn’t be achieved in this case due to the progressive worsened scenario of the case. The documentation of a primary source of malignancy wouldn’t have been missed if she presented earlier and the primary care physicians kept a high index of suspicion of a malignant process underlying the clinical picture of suppurative thyroiditis which she presented with. It is therefore recommended to consider, in the differential diagnosis, thyroid malignancy in any future case presenting with suppuration.
We acknowledge the support of the radiologist, Dr. Sarah Al-Mutawaa, and the pathologist, Dr. Shahed Pathan, who kindly assisted us in the interpretation of the radiological films and the fine needle aspiration, respectively.