Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Review Article - (2014) Volume 3, Issue 2
Thyroid cancer is a relatively uncommon disease within the pediatric population. It represents less than 3% of the cancers in children. It is exceptional before the age of 10, and the incidence increases in adolescents, with a difference between boys and girls leading to the preponderance of females affected by the disease similar to that observed in adults. By comparison, incidence rates in adults 20-24 years are 2.30/100 000 in men and 6.54/100 000 in women.
<Keywords: Epidemiology, Hyperthyroidism, Lymphadenopathies, Rhone alpes
Incidence of thyroid cancer in children and adolescents
The age-ajusted incidence rates collected from the French regional Rhone Alpes Registry (1998-2011) (RA-TCR) and from the Surveillance, Epidemiology and End Results registry (SEER) (1) are shown in Table 1. An annual increase of 1.1% in the incidence of pediatric thyroid cancers has been reported after a recent analysis of the SEER data collected over a long period of observation (more than 30 years ) [1]. In our experience spanning over a period of 13 years, there is no change in the incidence rates in the young population. This fact is in accordance with the stability of the incidence rates of the whole population of thyroid cancers in the Rhone Alpes region as reported in 2009 [2].
| Rhone Alpes BOYS | Rhone Alpes GIRLS | SEER BOYS and GIRLS | |
|---|---|---|---|
| 0-4 years | 0.04 | 0.13 | 0.10 |
| 5-9 years | 0.16 | 0.33 | O.16 |
| 10-14 years | 0.35 | 1.08 | 0.5 |
| 15-19 years | 1.03 | 3.52 | 1.33 |
Table 1: Incidence rates /100 0000
The frequency of each histological form in the RA-TCR is shown in tables (2a and 2b). The large predominance of the papillary cancers is similar to that found in the whole collection of cancers collected in the RA-RCT [2]. Papillary and follicular cancers are the most common types of well differentiated thyroid malignancies. The distribution of the papillary subtypes differs from that observed in the adults by a higher frequency of the diffuse sclerosing and the solid subtypes in young people.
| 2a | 2b | ||
|---|---|---|---|
| Papillary | 82% | Classic | 43% |
| Follicular | 5% | Follicular | 39% |
| Medullary | 8% | Medullary | 5% |
| Poorly differentiated | 4.80% | Poorly differentiated | 9% |
Table 2: 2a: Distribution of histological forms of thyroid cancers in children and adolescents, 2b: Distribution of the various subtypes of papillary cancers in the Rhone Alpes Thyroid cancer registry
Clinical characteristics of thyroid cancers in children and adolescents
The clinical manifestations of pediatric thyroid cancers at diagnosis are more aggressive than that of adult patients. Indeed, clinical lymphadenopathies are reported in 20-75%, extra thyroid extension in 20-50% and distant metastases, namely pulmonary in 7-25% of patients [3-8]. In our experience children have more signs of aggressiveness than adolescents (Table 3 and Figure 1). The prevalence of micro cancers in our series is 21% (N=35) in the whole group of children and adolescents (13 tumors in children and 22 in adolescents). These micro cancers correspond to various clinical conditions of diagnosis: 1-Discovery of a fortuitous cancer in half cases found in goiters, in hyperthyroidism, or associated to an adenoma. 2- Discovery of a microcancer after systematic prophylactic surgery in familial medullary carcinomas or after surgery in patients survivors after cervical radiotherapy for malignancy in childhood, carefully followed by cervical ultrasonography.
| Children (N=50) | Adolescent (N= 115) | |
|---|---|---|
| Metastatic cervical lymph nodes | 39% | 33% |
| Extrathyroid extension | 26% | 17% |
| Multifocality | 32% | 17% |
| Mean tumor size(cm) | 2.10 1.7 | 2.40+-1.6 |
Table 3: Characteristics of thyroid cancers in children and adolescents in the Rhone Alpes Thyroid cancer registry
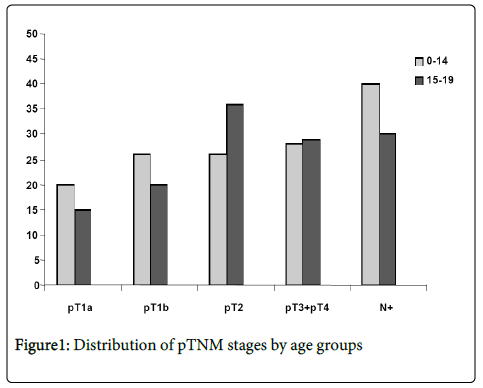
Figure 1: Distribution of pTNM stages by age groups
Surgical treatment consisted of total or near total thyroidectomy in most patients. IRA therapy was administered to 60% of the patients.
Despite the initial aggressiveness, the general prognosis of this cancer is favourable. Recent data [3,4] showed a survival rate of 98%, and recurrence rates of 35% [3,5]. The recurrences take place in most series during the 2 first years, namely the cervical metastatic lymph nodes leading to secondary resection. The presence of invaded lymph nodes at first surgery is the major risk factor for this recurrence [9]. In our experience, based on a limited number of patients i.e. 33 children and 73 adolescents with a mean follow up period of 6 years, the recurrences are rare (Table 4). All 5 children who had secondary cervical lymphadenopathy had metastatic nodes at initial surgery and thus had been submitted to neck dissection. Persisting illness consisted of lung metastases in 5 and persistence of elevated thyroglobulin in 1, as described in references [10,11]. In two adolescent patients, metastases became refractory after repeated IRA therapy. In the other 5 patients, persisting illness consisted of lung metastases and of recurrent lymphadenopathy after repeated surgery.
| Children N=33 | Adolescents N= 73 | |
|---|---|---|
| Cervical lymph node recurrence | 5/33 (15%) | 6/73 (8%) |
| Lung metastases | 7/33 (21%) | 6/73(8%) |
| Persisting illness at last evaluation | 6/33 (18%) | 7 /73 (9.5%) |
| Remission rate | 82% | 88% |
Table 4: Outcome events
Two factors have been evaluated as potentially unfavourable for the evolution of cancers: the previous cervical radiotherapy for another cancer in childhood and the presence of molecular oncogenic alterations in thyroid cancer. The results of these studies have been previously reported [10,11].
Radiations in childhood represent the major risk factor for thyroid cancer. In our experience 18% of the children and 7% of the adolescents with thyroid cancer had been submitted to radiotherapy for malignancy in childhood.
We do not have to date any data concerning other medical irradiations such as that provided by CT scans. A case control study was performed to evaluate the influence of previous radiotherapy on the initial presentation and on the evolution of the illness [10]. This study showed that radiation-associated thyroid cancers have a more aggressive initial profile, mainly when the cancer is diagnosed in early adulthood (Figure 2). Despite this less favourable initial presentation, the general prognosis of these cancers does not differ of that of the non-radiation–associated sporadic cancers matched on age, and tumor stage (Table 5).
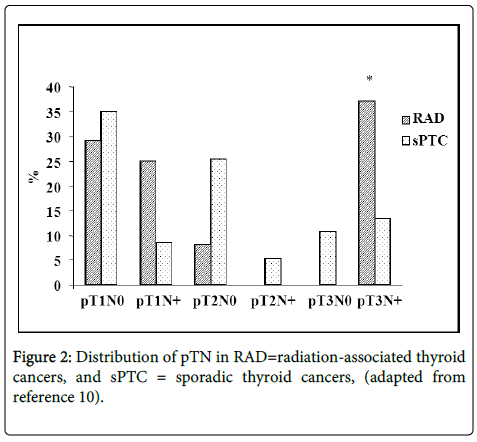
Figure 2: Distribution of pTN in RAD=radiation-associated thyroid cancers, and sPTC = sporadic thyroid cancers, (adapted from reference 10).
| RAD (Cases) | sPTC (Controls) | Odds ratio (95%CI) | |
|---|---|---|---|
| 8-14 years | |||
| Number | 11 | 22 | |
| Metastasis(es) at first evaluation | 0 | 0 | |
| Recurrence LNM | 2 | 5 | 0.75 [0.12-4.7] ns |
| 15-20 years | |||
| Number | 5 | 21 | |
| Metastasis(es) at first evaluation | 0 | 0 | |
| Recurrence LNM | 1 | 2 | 2.3 [0.17-33] ns |
| 21-29 years | |||
| Number | 8 | 37 | |
| Metastasis(es) at first evaluation | 1 | 3 | |
| Recurrence LNM | 0 | 6 | 0.4 [0.02-8.9] ns |
| All patients | |||
| Number | 24 | 80 | |
| Metastasis(es) at first evaluation | 1 | 3 | |
| Recurrence LNM | 3 | 13 | 0.73 [0.19-2.83] ns |
| pT3N+ | |||
| Number | 9 | 27 | |
| Metastasis(es) at first evaluation | 1 | 3 | |
| Recurrence LNM | 2 | 6 | 1 [0.16-6.14] ns |
Table 5: Risk of outcome events in RAD = radiation-associated thyroid cancers, and sPTC=matched sporadic thyroid cancers, according to the age subgroups, the whole groups and the high risk groups (pT3N+). (adapted from reference 10)
Molecular oncogenic alterations of the Map kinase pathway are found less frequently in the cancers of the young patients than in the adult tumors. They have been shown to increase with age, namely as concerns the Braf mutations which are exceptional in the cancer of young people. The experience of the RA TCR confirms this data showing an increase with age in the prevalence of these alterations (Figure 3) comparing the prevalence of these alterations in children adolescents to that in young adults as reported in ref [11]. It must be noted that Braf mutations which are present in more than 50% of thyroid cancers in adults are rare in the cancers of young people. The study shows that there is no difference in the evolution in relation with the presence or the absence of the oncogenic alterations of the Map kinase pathway in the children and adolescent tumors [11].The results of our study showed an impact of the presence of Ret/ PTC on the evolution of the cancer, only in the young adults population.
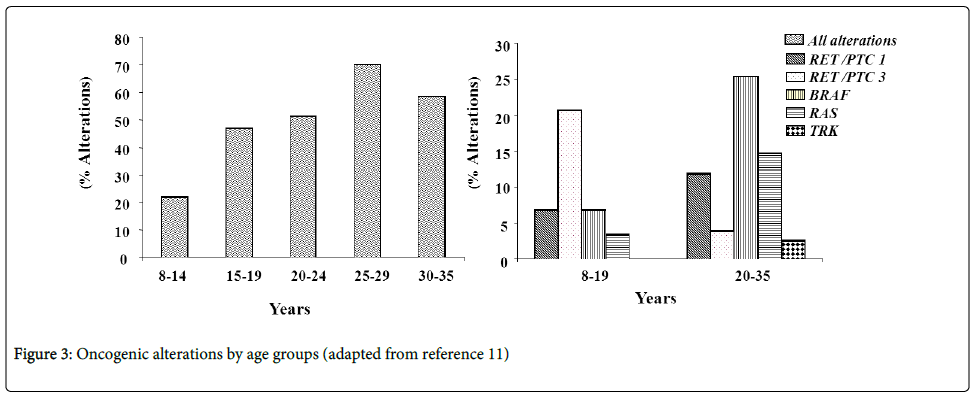
Figure 3: Oncogenic alterations by age groups (adapted from reference 11)
Thyroid cancers in children and adolescents are rare. They have a good general prognosis despite their initial presentation which is more aggressive than that of the adults with more metastatic diffusion namely in cervical lymph nodes. This prognosis does not seem to be influenced by previous medical, therapeutic exposure toX rays nor by the presence of oncogenic alterations of the Map kinase pathway.
The risk factors for this cancer of the young people, other than radiations and familial thyroid pathology, remain to be described.