Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2016) Volume 5, Issue 2
Introduction: Metastases to the thyroid gland are rare in clinical practice. 12 to 34% of secondary thyroid tumors originate from renal carcinoma. We report a case of late thyroid metastasis, eight year after a nephrectomy for clear cell renal carcinoma.
Case: A 70-years-old Caucasian patient followed for a multi-nodular goiter with a history of renal carcinoma, underwent a thyroidectomy. A histological examination revealed clear cell renal carcinoma metastasis to the thyroid.
Conclusion: Metastases to the thyroid gland are usually asymptomatic. The diagnosis of secondary malignant thyroid tumor should be taken into account if there is history of neoplasia, renal in particular, even years after the surgery of the primary tumor.
<Keywords: Late thyroid metastasis; Renal cell carcinoma; Nephrectomy
Localized malignant renal tumors requires a surgical intervention as first line treatment by partial nephrectomy, or if it is not feasible, by radical nephrectomy. The risk for recurrence after surgery is about 30 to 40%, with median delay time of 15 month [1]. Although the first metastatic site is pulmonary, it is not rare to observe some metastasis in other organs such as thyroid [2].
The renal origin of thyroid metastasis is an important prognostic indicator to consider, because it determines the therapeutic management of a patient. It has been demonstrated that these secondary sites could not be synchronous, and can occur until more than twenty years after the initial nephrectomy [3].
We report the case of a 70 year old patient followed for asymptomatic multi-nodular goiter diagnosed with a thyroid metastasis of renal carcinoma operated eight years ago.
A 70-years-old Caucasian patient was followed for a multi-nodular goiter and she had a past medical and surgical history of high blood pressure, a bilateral chronic glaucoma and a radical left nephrectomy for renal cell carcinoma.
Eight years after her renal surgery and during her multi-nodular goiter follow-up, we noted an increase of the size of a right lobe hyper vascularized nodule (3.8×2.8×2.5 cm). There were no cervical masses and no thyroid function abnormalities. A total thyroidectomy was performed.
The pathological examination showed a 2 cm nodule (Figure 1) with histological aspect of a clear cell carcinoma. The tumor, highly vascularized expressing CD10 (Figure 2) but not thyroglobulin (Figure 3). The histology and the immunochemical profile were compatible with a thyroid metastasis of a renal carcinoma.
Figure 1: Thyroid lobe with a 2 cm nodule.
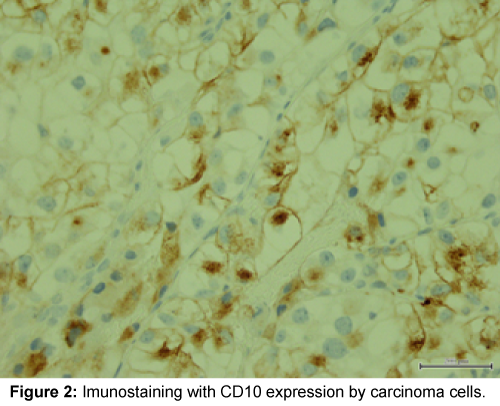
Figure 2: Imunostaining with CD10 expression by carcinoma cells.
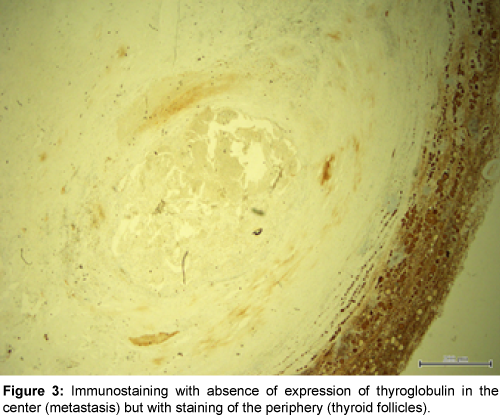
Figure 3: Immunostaining with absence of expression of thyroglobulin in the center (metastasis) but with staining of the periphery (thyroid follicles).
A long-term follow-up schema does not exist for patients who underwent nephrectomy for localized renal cell carcinoma (clear cell). The risk of local recurrence is always there. The French Association of Urology recommends biological surveillance of renal function, and a local recurrence monitoring of the disease using abdominal and renal CT with contrast, as well as screening of pulmonary metastasis by Chest CT scanning. However, rhythm and treatment modalities are not consensual and must be adapted to the evolving risk of the primary tumor [1].
There are some prognostic models developed to predict the occurrence risk of distant metastasis of surgery, but these models still less used, these recommendations are based on a low level of evidence.
Metastases to the thyroid gland are uncommon in current clinical practice. However, their incidence reported in autopsies series is high up to 24% of patients who die from malignancies [2].
Their character usually is asymptomatic and thus often, leads to underdiagnosis. Nevertheless, the presence of metastases is an important criterion to take into account for treatment of primary neoplasia.
In our case, we were able to diagnose the presence of metastases in this asymptomatic patient by clinical follow up and the presence of renal neoplasia history.
In conclusion, it seems important to consider the malignant tumor process such as metastasis than in any thyroid nodule found in a patient who was followed for neoplasia, renal in particular. The cancer history should be followed regularly for patients with a thyroid nodule and perform additional investigations in case of suspicion.
We declare no conflict of interests.