Journal of Depression and Anxiety
Open Access
ISSN: 2167-1044
ISSN: 2167-1044
Research Article - (2018) Volume 7, Issue 1
Background: Depression is a major public health problem, in terms of its prevalence and suffering, dysfunction, morbidity, and economic burden. Thyroid dysfunction is often seen in the patient with depression. Thyroid Function Test’s (TFT) can be considered as an integral part of the evaluation of newly depressed patients. Therefore, it will be beneficial for the psychiatrists to be cautious during the management of treatment resistant depression cases.
Aim: 1) To assess the thyroid profile in newly diagnosed drug naïve depression cases and healthy control and 2) To find out the clinical correlation between the thyroid profile and severity of depression.
Materials and Methods: It is a case control study where - Study group is newly diagnosed drug naïve case of depression and control group is the equal number of same age and sex matched people selected from the normal healthy population. Thyroid profile level is evaluated in both this group and levels are compared.
Results and Discussion: This study shows that the number of moderate and severe depression cases is more than the mild depression of cases and thyroid profile levels (T3, T4, and TSH) are increased with increasing severity of depression. A Maximum number of cases in study group show normal thyroid level (76%), only 2% of cases have hypothyroidism and 14% and 8% of cases have subclinical hypothyroidism and hyperthyroidism.
Conclusion: Many a time it has been seen that cases of depression show resistance to treatment and thyroid dysfunction are one the causes of such resistant cases. Therefore thyroid screening test is necessary for depression. Future prospective studies are needed, to clarify the significance of thyroid dysfunction in depression and help us to understand the etio-pathology and management of depression.
Keywords: Management; Severity; Resistant; Treatment
Mood disorders are the most common psychiatric disorder and in the most recent surveys, it has been seen that major depressive has the highest lifetime prevalence (almost 17 percent) of any psychiatric disorder [1]. The World Health Organization (WHO) estimated that about 100 million individuals develop depression every year [2]. It is seen that India has about 16.6 million new cases of major depression per year and 10.3 million cases at any time [3].
Even though depression is predominantly expressed through psychological symptoms, it is considered as a biological disorder and many times often it responds well to biological treatments [4].
It is seen that thyroid hormones have a profound influence on the human brain and behavior, and the interrelationship between thyroid dysfunction and psychiatric disturbances has always been well documented. Patients with thyroid disturbances can present with a variety of neuropsychiatric symptoms, including depressed mood, mania, acute psychosis, anxiety, and dementia [5].
T3 (Triioodothyronine) is available in peripheral organs and T4 (Tetraiodothyronine) is available in brain. T3 acts as a neuromodulator by enhancing γ-aminobutyric acid (GABA) release and calcium influx, which subsequently facilitate neurotransmitter release. It has been shown that to predict relapse in unipolar depression T3 levels is measured, and exogenous T3 supplementation appears to potentiate or accelerate the antidepressant response [6].
Although most depressed subjects have normal T3, T4 and TSH (Thyroid stimulating hormone) circulating levels, there is evidence of altered activity of the HPT (Hypothalamo Pituitary Thalamocortical) axis in some cases of depression including:
• The increase in the total and/or free T4, many times within the normality levels.
• The excessive response of TSH.
• High levels of ant thyroid antibodies present and
• High concentration of TRH in the cerebrospinal fluid of depressed Subjects [7].
Epidemiological surveys show that there is very high level of prevalence of hypothyroidism in Assam [8]. But there is a dearth of study of hypothyroidism and depression in North East India yet. Therefore this study is a sincere effort to see and analyse the thyroid profile level among unipolar depression cases so that it will improve our clinical judgment and management in cases of depression, especially the treatment resistant depression cases.
1. To assess thyroid profile in newly diagnosed drug naïve cases of depression and control group.
2. To find out clinical correlation between the thyroid profile and severity of depression
Study design
The study was a case control study. There were two groups, Group A is the study group. The cases included in group A were those patients who were diagnosed as DRUG NAIVE cases of DEPRESSION and who reported to the outpatient and inpatient department of psychiatry, Assam medical college, Dibrugarh. The study samples were selected from those patients who fulfilled the inclusion criteria and those who were not excluded. The total number of cases was 50. Group B is the control group and selected from a normal population of same age and sex, fulfilling the inclusion and exclusion criteria. The total number of the patient was 50.
Inclusion criteria
Study group (Group A)
• Newly diagnosed drug naïve cases of unipolar depression in >20 years to 60 years age group.
• Patients of both sexes.
• Diagnosed drug naive cases of depression (ICD-10) and confirmed by the senior consultant psychiatrist.
• Patients giving informed consent for the study.
Exclusion criteria
• Patients with diabetes, hypertension, stroke, renal, liver disorders, infection, the autoimmune disorder, known endocrine disorder and other psychiatric and patient with past history of mania.
• Patients on systemic drugs such as antipsychotics, anti-depressant, Oral contraceptive pill, substance use, anti-thyroid drugs/hormone replacement.
• Pregnant and lactating females.
Tools used
• Semi-structured Proforma developed and used in the Department of Psychiatry, Assam Medical College, Dibrugarh, Assam are mentioned in the Figure 1 below.
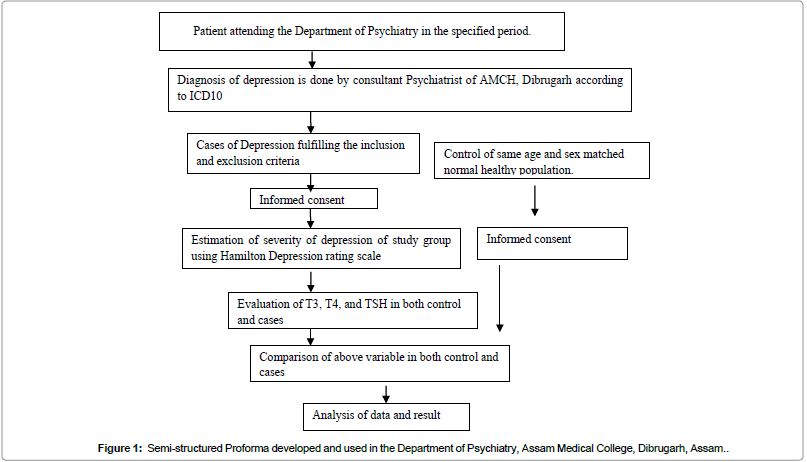
Figure 1: Semi-structured Proforma developed and used in the Department of Psychiatry, Assam Medical College, Dibrugarh, Assam..
• Kuppuswammy Scale for social class.
• ICD-10 Diagnostic Guidelines.
• Hamilton Depression Rating Scale.
All patients in the age group 21-60 years fulfilling the inclusion criteria for the study were included in the study. An informed consent was taken from each participant. Thyroid profile level (T3, T4, and TSH) of each participant were measured in RIA centre, AMCH. Similarly, same age and sex matched healthy control was selected and thyroid profile level were measured as shown in the below Figure 1.
At the end of 1-year data was collected from a total of 50 subjects with a diagnosis of Depression (ICD-10), they comprised the study group. Similarly, there were another 50 subjects who were age and sex matched healthy individuals belonging to the same socio-cultural background and they comprised the control group. As we had two separate groups with the proportionate number of cases, the statistical calculation was done in the two groups separately and comparison was made between them.
Tables 1-4 show that that the female subjects comprised a greater proportion of the sample size compared to male subjects in both the study and control group. The maximum number of married people (70%) has depression compared to unmarried people (28%). Most of the participants were Hindu by religion in both the study and control group (94% in the study group and 92% in control group). In contrast, a small proportion of subjects (4% in the study group and 6% in control group) were Muslim and only 2% in both the groups were Christian. In our study we have also found that person from nuclear family (72%) have more depression compared to joint family (28%); people from the urban area (52%) have more depression compared to rural area. The Person from lower middle-class socio-economic status (62%) has more depression compared to upper middle class (12%).
| Socio-demographic variables | Variables sub-group | Group a (depression) | Group b (control) | X2 | Df | P-value |
|---|---|---|---|---|---|---|
| Gender | Male | 21 (42%) | 20 (32%) | 0.413 | 1 | 0.839 |
| Female | 29 (58%) | 30 (68%) | ||||
| Religion | Hindu | 47 (94%) | 46 (92%) | 0.211 | 2 | 0.900 |
| Muslim | 2 (4%) | 3 (6%) | ||||
| Christian | 1 (2%) | 1 (2%) | ||||
| Others | 0 | 0 | ||||
| Marital status | Married | 35 (70%) | 41 (82%) | 2.56 | 2 | 0.277948 |
| Unmarried | 14 (28%) | 9 (18%) | ||||
| Widow | 1 (2%) | 0 | ||||
| Type of family | Nuclear | 36 (72%) | 28 (56%) | 5.50 | 2 | 0.064 |
| Joint | 14 (28%) | 18 (36%) | ||||
| Extended | 0 | 4 (8%) | ||||
| Domicile | Urban | 26 (52%) | 18 (36%) | 2.60 | 1 | 0.107 |
| Rural | 24 (48%) | 32 (64%) | ||||
| Socio-economic Status |
Upper | 0 | 0 | 1.41 | 2 | 0.495 |
| Upper middle | 6 (12%) | 10 (20%) | ||||
| Lower middle | 31 (62%) | 30 (60%) | ||||
| Upper lower | 13 (26%) | 10 (20%) | ||||
| Lower | 0 | 0 | ||||
| Education | Professor | 0 | 0 | 3.76 | 4 | 0.440 |
| Graduate | 0 | 0 | ||||
| Intermediate | 2 (4%) | 5 (10%) | ||||
| High school | 8 (16%) | 13 (26%) | ||||
| Middle school | 18 (36%) | 13 (26%) | ||||
| Primary | 11 (22%) | 8 (16%) | ||||
| Illiterate | 11 (22%) | 11 (22%) | ||||
| Occupation | Profession | 0 | 0 | 4.32 | 5 | 0.504 |
| Semiprofessional | 0 | 1 (2%) | ||||
| Clerical | 4 (8%) | 7 (14%) | ||||
| Skilled | 1 (2%) | 4 (8%) | ||||
| Semiskilled | 5 (10%) | 4 (8%) | ||||
| Unskilled | 7 (14%) | 5 (10%) | ||||
| Unemployed | 33 (66%) | 29 (58%) |
Table 1: Socio-demographic variables.
| Variables | T3 | T4 | TSH | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Group A | 1.139 | O.420 | 94.54 | 21.83 | 2.7086 | 1.8038 |
| Group B | 1.133 | O.5 | 90.14 | 20.617 | 2.44 | 1.28 |
| p-value | 0.9483 | 0.3027 | 0.3926 | |||
In Table 2 it is seen that both study group (A) and control group (B) have an almost similar level of thyroid profile level.
Table 2: Comparison of thyroid profile level between study group (Group A) and Control Group (Group B).
| Severity | No | Male | Female |
|---|---|---|---|
| Mild | 3 (60%) | 1 (2%) | 2 (4%) |
| Moderate | 24 (48%) | 8 (16%) | 16 (32%) |
| Severe | 23 (46%) | 12 (24%) | 11 (22%) |
It has been seen that female cases (58%) outnumbered the male cases (42%) and 4% and 2% of female and male respectively have mild depression.32% of female and 16% of male have moderate depression, on the other hand, 24% male and 22% of female have severe depression.
Table 3: Severity of depression and distribution among sex.
| Variables | Mild | Moderate | Severe | No | P-value |
|---|---|---|---|---|---|
| Normal | 2 (4%) | 19 (38%) | 17 (34%) | 38 (76%) | 0.430 |
| Hypothyroid | 0 | 1 (2%) | 0 | 1 (2%) | |
| Hyperthyroid | 0 | 0 | 0 | 0 | |
| Subclinical hypothyroid | 1 (2%) | 2 (4%) | 4 (8%) | 7 (14%) | |
| Subclinical hyperthyroid | 0 | 2 (4%) | 2 (4%) | 4 (8%) |
Among the depression cases, a maximum number of cases have normal thyroid level (76%), in contrast to 14% of cases that have subclinical hypothyroidism, out of which 8% have severe depression, 4%, and 2% have moderate and mild depression respectively. Hypothyroidism is seen in only 2% of cases and 8% of cases have subclinical hyperthyroidism. But there is no statistical significance.
Table 4: Various thyroid status and severity of depression.
It has been seen that there are many kinds of literature available in the same domain and there is variable result in every study and in our study also we have found the same. The present study is a sincere attempt to evaluate the clinical correlation of Drug naive cases of Depression and Thyroid profile. Considering these above-mentioned aim, it has been found that there was no significant difference of thyroid profile level in drug naive cases of depression (Tables 2-4).
In our study, we have found most of the people from the study group came from the nuclear family (72%) and 28% from the joint family. So from these data, it has been seen that in the married people and people from nuclear family suffered more Depression than the other group. Our findings are similar to the findings of Chopra and Ram, Das, Kamble [9-11]. In our study we have found more Hindu people in both study and control group, which is contrast to the study by Chopra and Ram as they found more Muslim people in their study, probably because of local people distribution in the study area [9].
In our study, we have found that there are more cases of Moderate (16%) and Severe (14%) Depression compared to mild depression (2%). Saxena also found the similar type of variation in their study, On the other hand there is some other study like Das, and Kamble where they had found the distribution of patients in the mild, moderate and severe categories were similar [10-12].
The T3 level in study group (1.139 ± 0.420) is more than the control group (1.133 ± 0.5), though there is no statistical significance. This finding in our study is similar to the finding of Das [10]. On the other hand there are some other studies like Saxena, Kamble, Orsulak, Wahby, Chopra, Ram and Jain where they have found that T3 level in cases of depression is less than the control group [9-15].
There is increasing level of T4 in study group (94.54 ± 21.83) compared to control group (90.14 ± 20.617) and it is similar to the study of Chopra and Ram, Das, Kamble, Wilson, Mulder and Joyce. But some study showed decreased level of T4 in the study group compared to control group, like Saxena and in another study, Wahby there is a normal level of T4. The possible explanation may be that total T4 level is elevated during the acute phase of depression and it is a compensatory phenomenon to help increase the catecholamine neurotransmission for the alleviation of depressive affect. It is assumed that the conversion of T4 to T3 may be defective in the depressive illness [9-12,14,16].
TSH is high in the study group (2.7086 ± 1.8038) compared to control group (2.44 ± 1.28), but there is no significance. Our study findings are similar to the findings of Wahby, Baumgartner A Gräf, Kürten, Meinhold, Saxena, Chopra and Ram, Das, Jain. But some study like Joffe, Levitt, Kamble et al. has found the normal level of TSH [9-12,14,15,17].
It has been seen that with increasing severity of depression the level of thyroid profile (T3, T4, and TSH) increases, but there is no statistical significance between severity of depression and thyroid profile level (T3, T4, and TSH). Our this finding is opposite to the finding by Saxena, Das where they had found low T3 and high TSH level with increasing severity. But our finding resembles some extent with the study by Kamble. This variability may be because of difference in severity of depression cases [10-12].
In our study most of the cases of depression have normal thyroid profile level (38%), 2% have hypothyroidism, 14% have subclinical hypothyroidism and 8% have subclinical hyperthyroidism. A similar type of finding is seen in the study by Jain, Wahby, Kamble, Saxena where he found the prevalence of subclinical hypothyroidism is more than the hypothyroidism. In another study by Das, they had found that hypothyroidism is more prevalent than subclinical hypothyroidism. There are many studies where thyroid profile level was found to be normal [10-12,14,15].
Many a time it has been seen that cases of depression show resistance to treatment and thyroid dysfunction are one the causes of such resistant cases. Till now there are many studies regarding the relationship between the thyroid profile and depression, but the variability of results have been seen across them. Future prospective studies are needed, to clarify the significance of thyroid dysfunction in depression and help us to understand the etio-pathology and management of depression.