Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2015) Volume 4, Issue 3
Background: Radiofrequency ablation has been reported to be effective and safe in reducing benign thyroid volume nodules. Most studies carried out so far were performed on a limited number of large nodules and often a subset of them required more than one single treatment.
Case report: We describe the case of 82-year-old woman with a very large volume thyroid nodule treated with a single session of thyroid radiofrequency ablation. After six months, the patient showed significant improvement of compression symptoms and significant volume reduction of 68% (from 152 mL to 48 mL).
Methods: To our knowledge, this is the first case report so far that proves the effectiveness and safety of radiofrequency ablation in such a large thyroid nodule.
Conclusions: Radiofrequency ablation is very effective technique for the percutaneous treatment of thyroid nodules. Further data are needed to define the effectiveness and the feasibility in treating large thyroid nodules.
<Keywords: Thyroid nodule; Nodular goiter; Radiofrequency
Laser ablation (LA) and radiofrequency (RF) are the main techniques used for thermal ablation of benign thyroid nodules. In the past two decades, an increasing number of studies confirmed their effectiveness in reducing the volume of thyroid nodules with a few side effects [1-3]. We describe a case of 82 year-old female patient with a very large thyroid nodule. Because of the patient’s age and several comorbidities, she was deemed unsuitable for thyroid surgery and eligible for a percutaneous thermal treatment. After her informed consent, the patient underwent percutaneous RF ablation therapy.
An 82 year-old female patient was hospitalized in the Internal Medicine Department at S.M. Goretti Hospital in Latina, Italy, for heart failure, chronic renal insufficiency and nodular goiter. She was discharged with pharmacological therapy consisting of cardio kinetic drugs and enoxaparin (4000 UI subcutaneous/day) for 15 days. One week after hospitalization, the patient showed evident signs of compression in the neck with dysphagia and dyspnea. Probably, the use of enoxaparin has caused an intra-nodular goiter hemorrhage with consequent increase the nodule volume and the above-mentioned compression (Figure 1). For this reason, due to the patient’s age and the pre-existing cardiac pathology (heart failure, NYHA class 3), the patient agreed to RF treatment after being thoroughly informed. The patient underwent fine needle aspiration of the nodule, which resulted in cytological benign (TIR-2), and evacuation of 20 mL of hemorrhagic fluid. After evacuation of the fluid component, a CT scan, performed in the same session after these maneuvers, showed a large nodule with a volume of 152 mL, located in the right thyroid lobe, shifting the trachea on the left side. Afterwards the patient underwent thermal therapy with RF technique. A 17-gauge needle and a mean voltage of 60 watts were used for thermal ablation procedure, performed with the “moving shot” technique [4]. The patient was discharged the same day of the procedure with no severe complications or side effects. Ultrasound examinations at 1 month and 6 months after RF showed significant volume reduction equal to 66 mL and 48 mL, respectively (Figure 2). The patient has had a complete disappearance of compressive symptoms since the first month after the treatment. Thyroid nodule remained stable until the last check carried out on the sixth month of follow up (Figure 3).
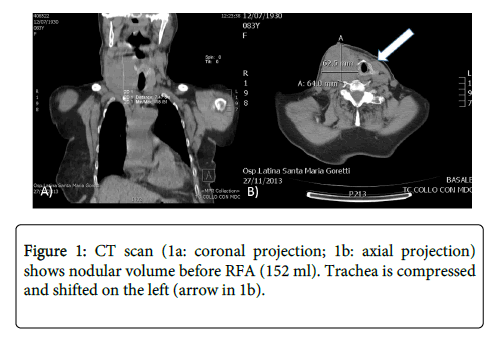
Figure 1: CT scan (1a: coronal projection; 1b: axial projection) shows nodular volume before RFA (152 ml). Trachea is compressed and shifted on the left (arrow in 1b).
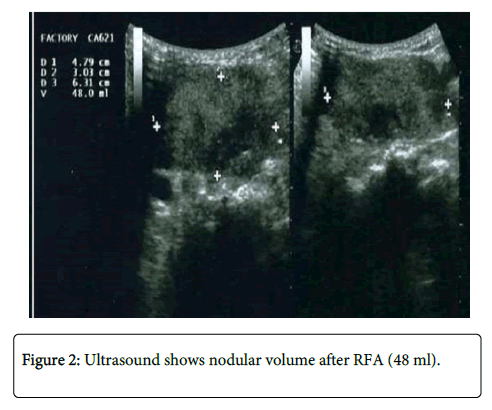
Figure 2: Ultrasound shows nodular volume after RFA (48 ml).
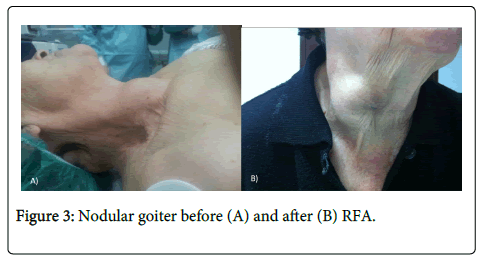
Figure 3: Nodular goiter before (A) and after (B) RFA.
Indications of RF ablation
Image-guided tissue ablation with both thermal and non-thermal sources has been used with favorable results in percutaneous treatment of benign thyroid nodules [1]. Thermal therapies such as RF, laser and microwave (MW), exploit interactions between tissue and energy which generates on the tip of the electrode needles to obtain temperatures which will cause irreversible damage to targeted cells (usually 50-54°C for at least 4-6 minutes). In the last decade, an increasing number of studies have also proven the effectiveness of RF ablation [5]. The above-mentioned methods should be aimed mainly for patients with compression symptoms and with strict contraindications to thyroid surgery. However these techniques could also be used in patients with nodules that although not significantly large, represent evident cosmetic problems. This information is even more relevant if we consider that, according to recent clinical data, levothyroxine therapy produces a significant size reduction in only a limited number of nodules while others continue to grow progressively [6-8].
Technique
The first experiences with RF were performed with 14-gauge devices equipped with expandable prongs (hook-umbrella) and a fixed electrode technique [9,10]. Dedicated, 18-gauge, straight-type internally cooled electrodes have been recently developed for thyroid lesions. After local anesthesia, with a trans-isthmic approach, the electrode is inserted from the isthmus into the targeted nodule. With a “moving shot” technique, multiple conceptual areas of the nodule are ablated unit-by-unit by moving the electrode tip under ultrasounf guidance [4,11]. The electrode is primarily positioned in the deepest part of the nodule, afterwards it is shifted laterally and across the isthmus. Once the needle is positioned the treatment starts by delivering radiofrequency energy (60 W) until a hyperechoic area (proving the necrosis) appears within the ablated area. The needle is then partially retracted and switched to another area of the nodule. If the hyperechoic area does not appear after 5 to 10 seconds, the power is increased of 10 W until a maximum of 100-110 W is reached. The treatment is considered completed when all the subunits of the nodule have been treated and show the classic post-ablation hyperechoic appearance. Recently, cooled electrodes of different thicknesses and lengths and various sized active points ranging from 0.5 to 1.5 cm are commercially available. In our center we use a 17 gauge needle (15 cm) with 1 cm active tip (Cool tip, Covidien, Ireland).
Previous findings
We recently reported the results of treatment with RF moving shot technique in nodules small (≥ 12mL) medium (from 12 to 30 mL) or large (> 30 mL) and we think that large nodules should be considered those that give a high score of cosmetic and symptoms compression [12]. It should be stressed that the nodules treated by the majority of authors who use moving-shot technique both in non-randomized and randomized studies have volumetric values ranging from 6 to 15 mL and a large fluid component in most cases [4,13-17]. In fact, there are only two randomized trial aimed to study the effect of RF in nodules with solid component greater than 80% of the baseline volume [4,16]. In addition, it is important to point out that the nodules with high fluid component need repeated RF treatment sessions, even up to seven times in some cases [14,15].
The nodule treated in this case report was very large even after the aspiration of the fluid component and nodule volume reduction was very significant (68%) after a single session of treatment with RF technique.
We believe that radiofrequency ablation is a promising technique for the treatment of benign thyroid nodules, even if they are large. However, further studies and longer follow-up periods are needed to confirm its safeness and effectiveness when large nodules, as in our case, are considered.
Consent
Written informed consent was obtained from the patient for publication of this Case Report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
R.C. and A.P. were the major contributors in writing the manuscript. V.P. and G.P. performed fine needle thyroid aspiration and R.F.A. G.C., A.P., A.C. and I.T. analyzed and interpreted the patient data regarding nodular disease and indication for RFA. All authors read and approved the final manuscript.