Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
![]() +44 1300 500008
+44 1300 500008
ISSN: 2167-7948
![]() +44 1300 500008
+44 1300 500008
Research Article - (2014) Volume 3, Issue 3
Background: Serum TSH is the target hormone by which adequate thyroid hormone supply can easily be monitored in patients with primary hypothyroidism. It is however controversial when TSH should be measured before thyroxine dose adjustments are made: 4 to 8 weeks are recommended. We looked at the time required to reach stable TSH levels in hypothyroid patients. Methods: We studied patients with newly diagnosed hypothyroidism (TSH >10 mU/l and fT4 <12.3 pmol/l). Treatment was initiated with thyroxine 50 μg/d if there was a history of cardiac disease and 100 μg/d otherwise. Blood pressure, weight and TSH, fT4, fT3, cystatin C and creatinine were measured once a week. Thyroxine dose was increased by 25 μg every 8 weeks until TSH normalised. Results: 12 patients with a mean TSH at baseline of 57.6 mU/l (range 11.3–151.8 mU/l) gave informed consent. They were followed for 8 to 24 weeks. After adjusting for the number of observation periods for each patient, the mean time to achieving stable TSH was 3.5 weeks (95% CI, 2.6-4.3 weeks), whereby stable TSH was defined as the value reached on a certain replacement dose after which TSH fluctuated by no more than +/- 2 mU/l during the remaining weeks of an 8 week observation period (median TSH at study end 4.7 mU/l). Conclusions: TSH did not change significantly after a mean of 3.5 weeks after the introduction of thyroxine. Dose changes can therefore be made after 4 weeks of treatment, longer periods are unnecessary.
<Hypothyroidism is defined as a condition in which the production of the thyroid hormones thyroxine (T4) and triiodothyronine (T3) by the thyroid gland is inadequate to meet peripheral tissue demand. Primary hypothyroidism is prevalent in up to 5% of the general population, with widely variable clinical symptoms. Thyroid failure caused by a disease of the thyroid gland is termed primary hypothyroidism. Primary hypothyroidism is by far the most common cause of hypothyroidism, and occurs as a result of Hashimoto’s thyroiditis, thyroidectomy, radiotherapy to the neck, radioiodine thyroid ablation or medications. Decreased levels of circulating free thyroxine and free triiodothyronine (fT4 and fT3) stimulate the production of thyroid stimulating hormone (TSH) in the pituitary gland to restore sufficient thyroid hormone production. An elevated serum TSH level is the main and most sensitive laboratory abnormality to occur in primary hypothyroidism, followed by reductions in serum levels of fT4 and fT3.
Synthetic levothyroxine is the treatment of choice for primary hypothyroidism. In Switzerland, two formulations are widely used, Eltroxin and Euthyrox. The average replacement dose of levothyroxine used in primary hypothyroidism is 1.6 µg/kg/d in young patients and 1.0 µg/kg/d in elderly subjects, who require a lower dose due to reduced thyroid hormone metabolism [1]. Elderly patients and those with heart disease may develop angina pectoris or arrhythmias when started on full replacement doses, as the heart rate and cardiac contractility improve with replacement and increase myocardial oxygen consumption. In such patients thyroid hormone replacement is usually commenced with 25 – 50 µg/d and increased gradually by 12.5 – 25 µg/d every 6 to 8 weeks [2].
To our knowledge, no study so far has investigated at which period of time levothyroxine dose adjustments can be made. The rationale behind the commonly used period of 6 to 8 weeks between dose adjustments is that changes in serum TSH levels lag behind changes in serum thyroid levels. Although fT4 levels increase rapidly once thyroxine supplementation is begun, the TSH response is much slower [3,4], in adults and neonates [5]. Recommendations for TSH screening intervals and thyroxine dose adjustments differ considerably, with the Swiss Pharmaceutical Compendium proposing TSH measurement and thyroxine dose adjustments, if necessary, every 2 – 4 weeks, the joint American Association of Clinical Endocrinologists (AACE) and American Thyroid Association (ATA) Guidelines every 4 – 8 weeks [6] and the British Thyroid Association Guideline advising 8 - 12 weeks [7].
Quality of life is affected by hypothyroidism and a rapid normalization of thyroid hormone levels is the primary aim of treatment. Previous studies have shown that many patients receive either excessive or insufficient supplementation [8]. On the other hand, unnecessarily frequent monitoring incurring substantial costs, possible risks to personal health (such as hematoma after phlebotomy) and posing an inconvenience to the patient should be avoided. Our aim was to better define after what length of time stable TSH levels in patients on thyroid hormone replacement are reached to guide and standardize treatment.
A further aspect of our study was the influence thyroid hormones on kidney function. It is well known that hypothyroidism decreases renal blood flow and creatinine clearance/GFR, as reflected by an increase in creatinine levels. We wanted to observe the changes in creatinine and cystatin C levels under the influence of thyroxine treatment. Because cystatin C is a more reliable marker of renal action than creatinine, we measured both creatinine and cystatin C on a weekly basis during the study.
Patients with newly diagnosed hypothyroidism (TSH >10 mU/l and fT4 <12.3 pmol/l) referred to the Department of Diabetes, Endocrinology and Clinical Nutrition at the University Hospital of Zurich were asked to participate in the study. Treatment was initiated with thyroxine 50 µg/d if there was a history of cardiac disease and 100 µg/d otherwise. Either Eltroxin or Euthyrox were prescribed. Ethical approval for the study was obtained in accordance with local institutional requirements. All subjects provided written informed consent. Data were collected between October 2010 and October 2011.
Blood pressure and weight were recorded at baseline and once a week thereafter on the same day or, if not possible, a day earlier or later, for 8 weeks. If TSH had not normalised after 8 weeks, the thyroxine dose was increased by 25 µg/d and blood pressure and weight were recorded once a week for a further 8 weeks. This cycle was repeated until TSH had normalized or the patient withdrew from the study.
Serum samples and laboratory assays
Blood samples were drawn once a week on the same day or, if not possible, a day earlier or later, either in the morning or afternoon. Patients were not fasting. Blood was taken for concentrations of TSH, fT4, fT3, creatinine and cystatin C. TSH, fT4 and fT3 were measured using an electrochemi-luminescence immunoassay (ECLIA) (Cobas 8000, e602 System from Roche Diagnostics). The assay for TSH had a sensitivity to 0.005 mU/l with a TSH analytic range from 0.005-100 mU/l (adult reference range 0.16 – 4.25 mU/l). The analytical measurement range for the fT4 assay was 0.3 - 100 pmol/l (adult reference range 12.3–20.2 pmol/l) and the measurement range for the fT3 assay 0.4-50 pmol/l (adult reference range 3.6 – 6.4 pmol/l).
The precision was assessed by measuring twenty replicates of quality control samples over 20 days. The coefficient of variation expressed as CV% was less than 2.5%, less than 4.9% and less than 3.9% for TSH, fT4 and fT3 measurements, respectively (covering a measuring range of 1.6-9.5 mU/l, 5.8-19.3 pmol/l and 16.1-37.6 pmol/l for TSH, fT3 and fT4 respectively).
Creatinine was measured using the Jaffe-Method (Cobas 8000, c701 System from Roche Diagnostics; coefficient of variation was 2.4% at 95 µmol/l and 2.3% at 337 µmol/l) and cystatin C by immune nephelometry (Behring Nephelometer by Dade Behring; coefficient of variation was 5.9% at 0.97 mg/l and 4.8% at 1.86 mg/l).
Statistical analysis
The 12 patients were observed for a minimum of 8 weeks and a maximum of 24 weeks (8 patients for 8 weeks, 1 patient for 16 weeks and 2 patients for 24 weeks). One observation period corresponded to 8 weeks, during which the thyroxine replacement dose remained unchanged, resulting in 19 observation periods in the 12 patients. A stable TSH was defined as the value reached on a certain replacement dose after which TSH fluctuated by no more than +/- 2 mU/l during the remaining weeks of the observation period. Examples visualizing the definition of TSH stability are given in Table 1.
| Patient ID | Time (weeks) | TSH (mU/I) |
|---|---|---|
| Patient 3 | Baseline | 151.8 |
| 1 | 51.9 | |
| 2 | 25.7 | |
| stable TSH as per study protocol | 3 | 4.7 |
| 4 | 2.7 | |
| 5 | 1.1 | |
| 6 | 0.9 | |
| 7 | 0.6 | |
| 8 | 0.7 | |
| Patient 5 | Baseline | 11.2 |
| 1 | 5.6 | |
| stable TSH as per study protocol | 2 | 3.7 |
| 3 | 2.6 | |
| 4 | 2.4 | |
| 5 | 3.2 | |
| 6 | 2.8 | |
| 7 | 2.9 | |
| 8 | 2.1 | |
| Patient 12 | Baseline | 29.5 |
| 1 | 8.2 | |
| stable TSH as per study protocol | 2 | 4.5 |
| 3 | 5.5 | |
| 4 | 3.9 | |
| 5 | 3.5 | |
| 6 | 3.1 | |
| 7 | 2.7 | |
| 8 | 2.3 |
Table 1: Patient examples (stable TSH levels as defined per protocol highlighted in red)
We performed a regression analysis to define the mean time per patient required to reach stable TSH levels. To adjust for the different number of observation periods per patient we calculated weighted mean (95% confidence) values.
Paired t-tests were performed comparing patient characteristics at baseline and study end.
To further evaluate the association between thyroid parameters (TSH, fT4 and fT3) and kidney parameters (creatinine and cystatin C), we performed a multilevel regression analysis to control for potential confounders (age, weight, sex, creatinine) and to control for a potential cluster effect (e.g. taking into account repeated measurements per patient).
TSH levels
Twelve (6 male) patients, 44.6 + 11.6 (mean + SD; range 28 - 58) years old with a mean TSH at baseline of 59.8 mU/l (range 11.3 to 151.8 mU/l) gave informed consent and were included in the study. Patients characteristics as well as values at baseline and at final visit are summarised in Table 2.
| Variable | Baseline | final visit | p-value |
|---|---|---|---|
| mean (range) | mean (range) | ||
| Weight (kg) | 86.6 (56-126) | 88.7 (55-127) | 0.0095 |
| Systolic blood pressure (mm Hg) | 124.7 (100-156) | 124.8 (96-156) | 0.99 |
| Diastolic blood pressure (mm Hg) | 81.9 (66-95) | 79.6 (59-111) | 0.53 |
| Pulse (bpm) | 71 (54-88) | 71 (55-90) | 0.95 |
| TSH (mU/I) | 59.8 (11.3-151.8) | 4.7 (0.21-21.1) | 0.0014 |
| fT4 (pmol/I) | 6.3(1.9-10.8) | 18.0 (11.0-25.2) | 0.0001 |
| fT3 (pmol/I) | 2.8 (1.2-4.5) | 4.7 (3.4-6.2) | 0.0005 |
| Creatinine (mol/I) | 83.6 (58-176) | 82.3 (58-150) | 0.78 |
| Cystatin C (mg/I) | 0.75 (0.47-1.28) | 0.85 (0.55-1.33) | 0.0021 |
Table 2: Characteristics of the patients at baseline and after thyroxine replacement therapy
Nine patients were hypothyroid secondary to autoimmune disease (Hashimoto), 2 patients following total thyroidectomy and 1 patient following radiotherapy to the neck. 9 patients were euthyroid by the end of the study; the remaining 3 patients could not participate for a further 8 weeks due to work responsibilities.
Statistical analysis including all 19 observation periods revealed a mean time to achieving stable TSH after a thyroxine dose adjustment of 3.5 weeks (95% CI, 2.6 - 4.3 weeks). When patients 4, 7 and 8 were excluded, who each missed one follow-up appointment (patient 4 in week 4, patient 7 in week 3 and patient 8 in week 5) thus making the determination of TSH stability inaccurate, then the mean time to achieving stable TSH levels decreased further to 2.9 weeks (95% CI, 2.0 - 3.6 weeks). Figures 1 and 2 illustrate the changes in TSH and fT4 levels over time in all 12 patients.
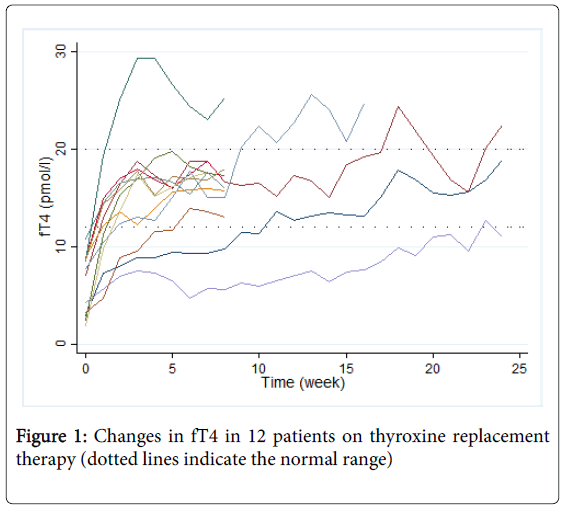
Figure 1: Changes in fT4 in 12 patients on thyroxine replacement therapy (dotted lines indicate the normal range)
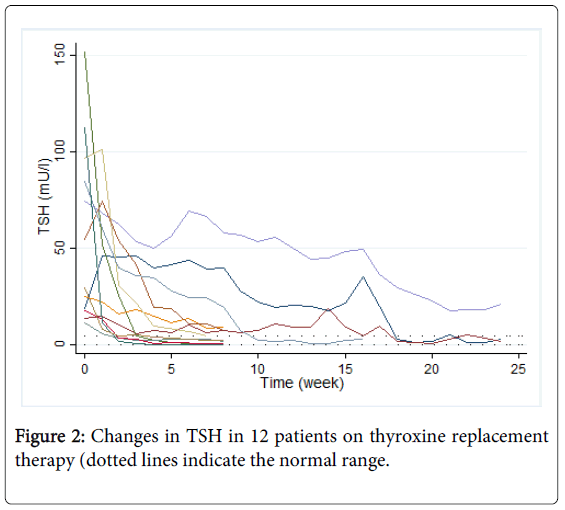
Figure 2: Changes in TSH in 12 patients on thyroxine replacement therapy (dotted lines indicate the normal range.
Table 3 shows the time needed to achieve stable TSH levels among all 12 study patients.
| Patient | Thyroxine dose (µg/d) | Stable TSH as per protocol (mU/l) | Time needed to reach stable TSH (weeks) |
|---|---|---|---|
| 1 | 50 | 39.8 | 4 |
| 75 | 19.6 | 3 | |
| 100 | 1.2 | 3 | |
| 2 | 100 | 10.2 | 3 |
| 125 | 7.5 | 2 | |
| 150 | 1.8 | 2 | |
| 3 | 100 | 4.7 | 4 |
| 4 | 100 | 8.5 | 7 |
| 5 | 100 | 3.7 | 3 |
| 6 | 100 | 3.8 | 3 |
| 7 | 100 | 56.6 | 5 |
| 125 | 44.2 | 5 | |
| 175 | 17.8 | 5 | |
| 8 | 100 | 4.6 | 7 |
| 9 | 100 | 11.2 | 6 |
| 10 | 100 | 24.5 | 6 |
| 150 | 2.2 | 2 | |
| 11 | 100 | 1.7 | 3 |
| 12 | 100 | 4.5 | 3 |
Table 3: Time needed to achieve stable TSH levels among the 12 study patients
Weight, blood pressure and pulse rate
Comparisons of patient’s characteristics between study beginning and end are presented in Table 2. Mean weight at baseline was 86.6 kg (range 56-126 kg). During the study, patients gained an average of 2.1 kg (95% CI 3.6 - 0.6 kg), which was statistically significant (p=0.009). Systolic blood pressure increased by 0.08 mm Hg and diastolic blood pressure decreased by 2.25 mm Hg from the beginning to the end of the study. Blood pressure changes did not reach statistical significance, neither did changes in pulse rate (p=>0.5 for all three parameters).
Creatinine and cystatin C
Mean creatinine at baseline in the 12 patients was 84 µmol/l (range 58 – 176 µmol/l) and 83 µmol/l (range 58–150 µmol/l) at study end. Paired t-tests showed no statistically significant change in creatinine following thyroid hormone replacement (p = 0.7). Mean cystatin C at baseline was 0.75 mg/l (range 0.47 – 1.28 mg/l) and 0.85 mg/l (range 0.55 – 1.33 mg/l) at study end, as illustrated in Table 2. The difference in cystatin C between patients was not significant. Multilevel regression analysis looking for potential effects of thyroid hormone parameters on kidney parameters revealed that cystatin C was significantly negatively associated with the TSH level (p=0.002), as shown in Figure 3.
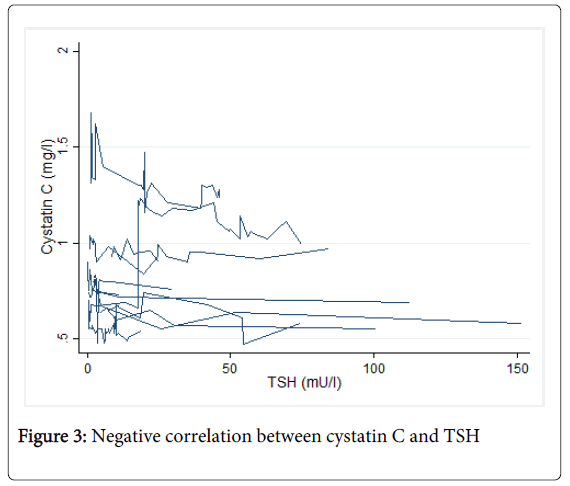
Figure 3: Negative correlation between cystatin C and TSH
In patients with an intact hypothalamic pituitary axis, the adequacy of thyroid hormone replacement can be assessed with TSH measurements. There is a precise feedback loop between circulating thyroid hormone and pituitary TSH secretion, with an exponential TSH increase after a decrease in fT4: a decrease in fT4 by a factor of 2 leads to an increase in TSH by a factor of about 100. Because of this sensitivity, TSH is a much better detector of minimal primary thyroid failure than the thyroid hormones [9]. However, although the half-life of TSH is short, the state and function of thyrotrope cells in the pituitary lag behind changes in serum thyroid hormone levels, so that the decrease in TSH values in response to thyroid hormone replacement treatment is delayed. In addition, TSH exerts its action at the transcription level and influences the hypertrophy and hyperplasia of follicular cells. These adaptive responses result in a prolonged elevation of TSH levels, so that the full effect of thyroid hormone replacement on TSH does not become apparent for a number of weeks [10,11].
To date, many guidelines for thyroid function testing and thyroid hormone adjustment by a number of professional societies have been published, and because of the relatively slow response time of the pituitary, most organisations recommend repeat measurements of TSH and adaption of thyroxine doses every 4 to 12 weeks. Once a stable maintenance dose of thyroxine with a TSH level within the reference range has been reached, subsequent TSH measurements are generally only required once a year [12].
Both excessive as well as insufficient thyroxine replacement is detrimental to a patient and may be associated with substantial deleterious effects on quality of life. Thyroid hormone has profound effects on the central nervous system, cardiovascular system, lipid profile, bone metabolism and structure, energy expenditure, and body weight. Consequently, hypothyroid patients may complain of cognitive deficit, mood alteration and weight gain [13,14], whereas the negative effects of excessive thyroxine replacement on bone metabolism, cardiac function, skeletal muscle and the brain are well known. Defining the time at which TSH measurement and thyroxine dose adjustment during titration of thyroid replacement therapy is reasonable and will reliably mirror a steady state is important, and guidelines for physicians are published at regular intervals [15-19]. The current recommended range of 4-12 weeks seems wide and varies considerably between specialist guidelines.
This study, although small, clearly suggests that a steady state in TSH levels after a change in thyroxine dose is reached after approximately 3.5 weeks, with no major decreases in TSH >2 mU/l thereafter. Therefore, measuring TSH every 4 weeks and adjusting thyroxine dose at that time seems optimal. Knowing that dose adjustments after 4 weeks are safe and do not bear a risk of overtreatment will facilitate the care of hypothyroid patients, for whom prompt normalizations of TSH levels may improve general wellbeing. Three of our twelve patients did not continue with the study until TSH had normalized completely due to work responsibilities. One of these patients had a TSH level of 21 mU/l after 24 weeks of treatment, when he asked to discontinue with the study protocol, the other two patients had TSH levels of 7 mU/l and 9 mU/l respectively after 8 weeks of treatment according to study protocol. The patient with a minimum TSH of 21 mU/l had a body weight of 106 kg, and the starting dose of 50 µg of thyroxine with dose adjustments of 25 µg every 8 weeks will have been inadequate. TSH levels reached a nadir within every 8 week observation period after 5, 4 and 4 weeks, respectively, in line with the results seen among the other 11 patients.
Our study has limitations, the most major of which being the small number of patients included and the 3 patients who failed to complete the study according to protocol, resulting in a substantial proportion (25%) of patients lost to follow up. However, we feel our observation that TSH levels stabilise after approximately 3.5 weeks following a thyroxine dose adjustment is relevant to clinical practice and warrants confirmation in a larger study.
Patients in this study gained an average of 2.1 kg during follow-up. Six patients gained 1-2 kg and 2 patients lost 1 kg. Four patients (patients 1, 2, 7 and 10) experienced a significant weight gain of 4-6 kg. This weight gain is contrary to what would be expected when thyroxine replacement is begun. However, the 4 patients with significant weight gain became hypothyroid following thyreoidectomy for head and neck cancer as well as following thyroidectomy for severe amiodarone induced hyperthyroidism. These patients’ clinical condition improved considerably following the intervention, and improved well-being may have contributed to the observed weight gain. As weight gain is distressing for most patients, counteracting it with adequate thyroid hormone treatment is an argument in favour of thyroxine dose adjustments at the earliest feasible time.
Previous studies have shown that primary hypothyroidism is associated with changes in kidney function and promotes endothelial dysfunction [20-23]. Hypothyroidism decreases renal blood flow and creatinine clearance/GFR, as reflected by an increase in creatinine levels. Thyroid hormones have direct effects on blood vessels as well as indirect effects mediated by IGF-1 and VEGF. IGF-1 is known to increase forearm blood flow and creatinine clearance in humans and as hypothyroidism leads to low levels of IGF-1, creatinine clearance is in turn reduced. Cystatin C is considered a more reliable marker of kidney function than creatinine, as it is produced by most nucleated cells at a constant rate, is freely filtered by the glomeruli and completely reabsorbed and catabolised by the tubular cells and has a low interindividual variability. Compared with creatinine, cystatin C is less dependent on race, and is not correlated to lean tissue mass, gender or age. However, cystatin C is significantly affected by even mild thyroid dysfunction, and reacts more sensitively to hypo- and hyperthyroidism than creatinine, as the production rate of cystatin C is influenced by thyroid hormones [24]. Previous studies have shown that cystatin C significantly increases following thyroxine replacement in hypothyroid patients [20], a finding we can confirm in this study. Although creatinine did not decrease with T4 replacement therapy to a significant extent, our results showed a statistically significant increase in cystatin C levels following treatment (Table 2). However, the association between cystatin C and TSH is weak and becomes significant only when clustering (patients individual time course) is considered. The corresponding regression model, controlling for repeated measurements (n=135 cystatin C measurements in 12 subjects, n average=11.3 measurements) results in a significant negative association between cystatin C and TSH. This association remains unchanged when further controlled for age, weight, sex and creatinine (Figure 3). In conclusion, thyroid function has to be considered when cystatin C is used as a marker of kidney function.
We did not see a statistically significant change in diastolic blood pressure as a marker for endothelial dysfunction following thyroid hormone replacement therapy in this study, but a trend for an only non-significant reduction by 2.25 mmHg (p=0.5).
In conclusion, we found that stable TSH levels, defined as no further change in TSH levels >2 mU/l during the following weeks on the same thyroxine replacement dose, occurred after 3.5 weeks. With these results, measuring thyroid hormones and adapting thyroxine doses every 4 weeks in newly diagnosed hypothyroid patients seems reasonable.