Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2013) Volume 2, Issue 3
Background: Tracheal cysts are rare and usually present in children. The most common explanation for the etiology of these cysts suggests a congenital malformation due to ventral foregut folding. Tracheal cysts are typically not of great consequence to patients, however in many instances it is recommended that they be removed.
Methods: A chart review of a single patient was performed.
Results: A 35 year-old female with cystic fibrosis and a history of medullary thyroid cancer status post thyroidectomy and central neck dissection was found to have two hypoechoic nodules in the thyroid bed 21 months after surgery. Fine-needle biopsy showed pseudostratified ciliated epithelium in one nodule and a CT scan identified a previously absent tracheal cyst. Because the patient had undergone previous neck imaging for her preexisting conditions, it is known that her cyst developed post thyroidectomy.
Conclusion: The development of the tracheal cyst may be related to her other conditions and history of surgery although this is not possible to definitively prove. Development of hypoechoic ultrasound lesions in a patient with thyroid carcinoma can be worrisome. There are no similar reported cases in the literature and the clinician should remain aware of unusual masses presenting in the thyroid bed after thyroid carcinoma resection that may mimic recurrent thyroid carcinoma.
<Keywords: Thyroid cancer; Tracheal cyst; Cystic fibrosis
Tracheal cysts, also known as bronchogenic cysts, are a relatively unusual finding. Those reported are usually located within the mediastinum; however they are not typically located in the neck [1]. They are most commonly found in children, but can rarely be found in adults. They are generally thought to be a byproduct of a congenital malformation [2]. We herein report a tracheal cyst presenting as a thyroid bed mass suspicious for recurrent medullary thyroid carcinoma in a patient with cystic fibrosis. Relationship to previous thyroid surgery suggests an etiology other than congenital origin.
A 35 year-old female with cystic fibrosis and CF-related diabetes mellitus was diagnosed with a T2N0M0 medullary thyroid carcinoma located in the left lobe. She underwent total thyroidectomy, left central neck dissection, and left lateral neck dissection. Her primary tumor was 3.2 cm in greatest dimension, and nodes were negative for carcinoma. Genetic testing for RET proto-oncogene was negative. Her preoperative calcitonin was 38 and postoperatively her calcitonin remained consistently undetectable and CEA was low. Approximately 21 months after surgery, a routine surveillance ultrasound detected two hypoechoic nodules in the right inferior thyroid bed measuring 0.8×1.0×1.1 cm and 0.6×0.5×1.0 cm with microcalcifications but without doppler blood flow (Figure 1). Serum calcitonin levels continued to beundetectable, therefore the patient did not immediately want to undergo a biopsy. Repeat ultrasound 4 months later revealed three hypoechoic nodules with micro calcifications and minimal to no doppler blood flow in the right thyroid bed measuring 1.2×0.9×1.0 cm, 1.1×1.0×0.9 cm, and 0.5×0.4×0.8 cm. Ultrasound-guided fine needle aspiration biopsies were negative for malignancy and concurrent calcitonin washings were less than 5.0. The pathologist did note “rare bronchial cells” on one needle pass of the most superior of the three nodules. A repeat ultrasound 8 months later showed no change in the nodules. Serum CEA remained stable at 2.1 and calcitonin was again undetectable. To help further define the nodules, a soft tissue neck CT scan of the neck with and without contrast, revealed a 3.6×0.6 cm tracheal cyst along the right posterolateral trachea within the thyroid bed (Figure 2 and 3). This cyst correlated with the previously seen right thyroid bed nodule on ultrasound. No other pathologically enlarged nodules or lymph nodes were identified. We elected to monitor the cyst with a repeat CT scan in 6-9 months. She remains asymptomatic.
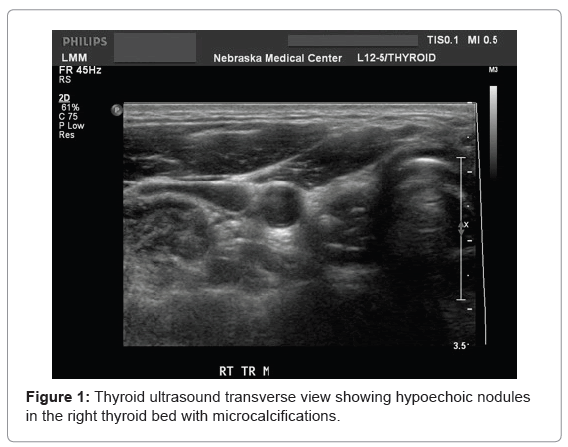
Figure 1: Thyroid ultrasound transverse view showing hypoechoic nodules in the right thyroid bed with microcalcifications.
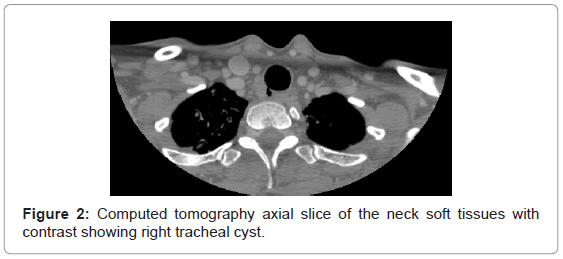
Figure 2: Computed tomography axial slice of the neck soft tissues with contrast showing right tracheal cyst.
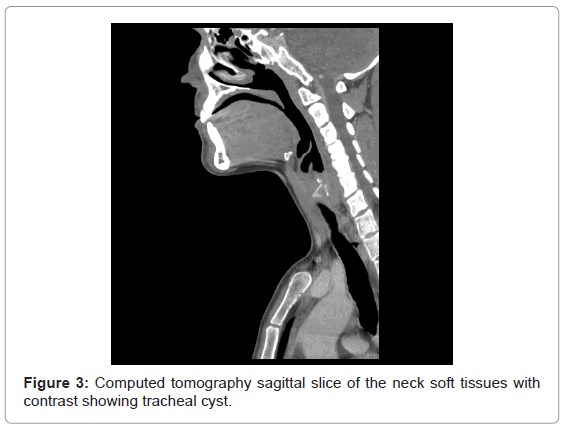
Figure 3: Computed tomography sagittal slice of the neck soft tissues with contrast showing tracheal cyst.
Of note, 3 weeks prior to her thyroidectomy and again 5 months afterwards she was admitted to the hospital for an exacerbation of her cystic fibrosis requiring IV antibiotics and intensification of her nebulizer therapy. During these periods, she experienced increased and prolonged episodes of coughing. Her past medical history was otherwise unremarkable and she had no family history of similar conditions. Her medications at the time of her CT scan included levothyroxine, calcium, and calcitriol.
Tracheal cysts are thought to be the result of a rare congenital malformation of the ventral foregut during embryological development [1,3]. Most commonly, these tracheal cysts are of no consequence to the patient. They are most frequently discovered in children, but in rare instances they may present in adults [4]. These cysts are usually found in the lung parenchyma or the mediastinum, although there are a few reported cases of occurrence in the cervical region. The most common differential diagnoses of these masses include thyroglossal duct cysts, parathyroid cysts, thyroid cysts, cervical thymic cysts, cystic hygromas, dermoid cysts, teratomas, and cystic neuromas [5]. Although tracheal cysts are typically asymptomatic in presentation and have minor consequences, in rare instances these cysts can become malignant, and may require surgical removal [6,7].
Instances of cervical tracheal cysts reported in the thyroid or perithyroidal region are quite unusual, with only a few known cases presented in the literature [8-11]. In the presented case, this finding was quite unexpected given that this cyst was not evident on neck ultrasound prior to surgery, during intra operative examination, or on neck ultrasound postoperatively for the first 2 years after surgery. The cyst developed or became apparent as an adult nearly 2 years after her total thyroidectomy and left central neck dissection. The cyst appearance also occurred during a year in which she had increased cystic fibrosis exacerbations and increased occurrence of prolonged coughing.
There are no existing reports of the presence of a tracheal cyst presenting itself post-thyroidectomy. Additionally, there are no published reports of para tracheal cysts occurring in conjunction with cystic fibrosis. One possible etiology of this patient’s cyst is a pre-existing congenital abnormality of the tracheal wall that did not present itself until adulthood, after she had undergone her thyroidectomy. Another possible cause includes surgical trauma to the tracheal adventitia allowing a congenital weakness in the submucosa to billow outwards between tracheal rings, although this seems less likely as the central neck dissection was targeted towards the side of the tumor on the left, contralateral from where the cyst was found. Other possibilities include weakening of the tracheal wall due to recurrent carcinoma or excessive intraluminal pressure with coughing secondary to her cystic fibrosis. Ultimately, the underlying etiology of her tracheal cyst is unknown.
This case illustrates an unusual presentation of a tracheal cyst in a patient with cystic fibrosis, and a history of medullary thyroid carcinoma status post total thyroidectomy. This tracheal cyst presented as a hypoechoic lesion in the thyroid bed causing suspicion for recurrent thyroid carcinoma. Suspicion for recurrent thyroid cancer is what makes report of this case important since awareness of this atypical presentation could save a patient from unnecessary surgical exploration. Hypoechoic lesions in the thyroid bed post thyroidectomy do not always represent cancer recurrence and in the setting of undetectable serum tumor markers other etiologies should be considered. In this case, we were able to identify the tracheal cyst by CT of the neck when ultrasound was not conclusive. The clinical follow up of thyroid cancer does not always include a CT of the neck, but this is a case where it served as a helpful adjunct. This case underscores the importance of evaluating all the clinical information when working up hypoechoic lesions in the thyroid bed following total thyroidectomy for thyroid cancer. If additional workup does not indicate thyroid cancer recurrence, then further evaluation for other etiologies is indicated.