Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Case Report - (2018) Volume 7, Issue 1
Cardiovascular manifestations of carbon monoxide (CO) poisoning in previous reports included pulmonary edema, heart failure, arrhythmia, and myocardial infarction. Herein, we report a 57 year old woman case of stressinduced cardiomyopathy (sCMP) related to CO poisoning with serial changes in EKGs and TTEs but delayed evolution of EKG recovery. And clinician should keep in mind that delyed recovery of EKGs could exist and serial EKG after full recovery of TTE finding.
Keywords: Carbon monoxide; Stress-induced cardiomyopathy; Delayed recovery
Cardiovascular manifestations of carbon monoxide (CO) poisoning in previous reports included pulmonary edema, heart failure, arrhythmia, and myocardial infarction [1]. As described in previous report [2], CO-induced cariomyopahty (CMP) and stress induced CMP (sCMP) share many common factors and similar clinical courses. In this report, we presented a case of sCMP related to CO poisoning, mimicking apical hypertrophic cardiomyopathy with somewhat different clinical course in usual sCMP
A 57-year-old woman was evaluated in the emergency room (ER) because of altered mental status. She had been exposed to carbon monoxide from a heater at home. She was found by a neighbor with altered mental status in her house. She had a medical history of wellcontrolled hypertension and postmenopausal osteoporosis, but no previous cardiac symptoms. On initial physical examination, she was drowsy, with Glasgow Coma Scale score of 12, and had decreased motor power in the upper and lower extremities. Blood pressure was 104/65 mmHg, heart rate was 93 beats/min, respiratory rate was 20 times/min, and initial O2 saturation was 100%. Arterial blood gas analysis and CO-oximetry were performed. The carboxyhemoglobin (COHb) level was 23.1% and oxygenated hemoglobin (O2Hb) was 77.1%. We diagnosed CO poisoning. Because of her drowsiness, we performed brain magnetic resonance imaging (Br-MRI). Br-MRI revealed acute stage infarction in the right pallidus. Although an initial EKG revealed regular sinus rhythm without ST segment changes (EKG1), levels of cardiac enzymes were elevated, with highly-sensitive troponin I 591.7 pg/mL, creatine kinase (CK)-MB 44.3 ng/ml, and total CK 1,618 IU/L. She was given oxygen 15 L/min via reservoir bag for treatment of CO poisoning. COHb decreased to 0% by the second hospital day and she recovered alertness. However, follow-up EKG demonstrated ST elevation in leads V2-V4 and T-wave inversion in leads V2-V6 (Figure 1A). To evaluate cardiac manifestations of CO poisoning, TTE was performed and showed akinesia at the apex and preserved wall motion in the mid-to-basal segments of the left ventricle (LV), with 48% ejection fraction (Figure 1B). To rule out acute coronary syndrome, we performed coronary angiography (CAG) with an ergonovine provocation test. CAG showed no luminal narrowing, plaque rupture, or spasm (Figure 1C and 1D).
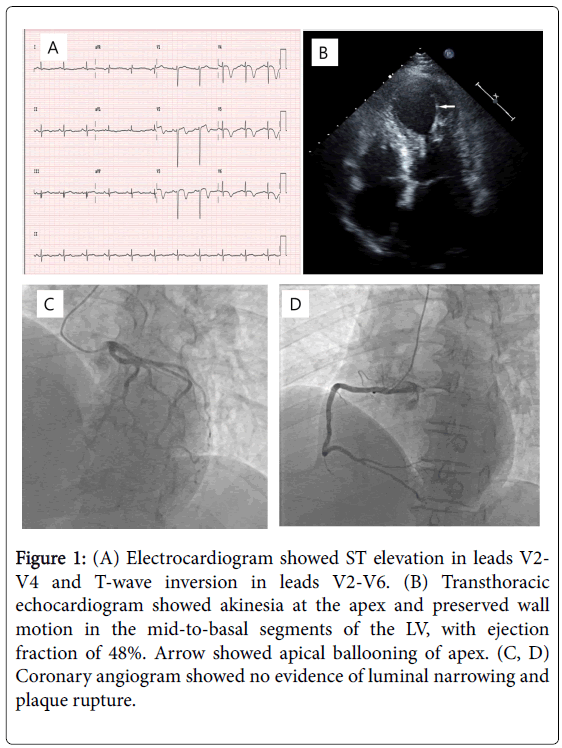
Figure 1: (A) Electrocardiogram showed ST elevation in leads V2- V4 and T-wave inversion in leads V2-V6. (B) Transthoracic echocardiogram showed akinesia at the apex and preserved wall motion in the mid-to-basal segments of the LV, with ejection fraction of 48%. Arrow showed apical ballooning of apex. (C, D) Coronary angiogram showed no evidence of luminal narrowing and plaque rupture.
We suspected sCMP related to CO poisoning, and provided conservative management. We performed TTE 1 week later (Figure 2B) The ejection fraction recovered to 63%, with improvement of regional wall motion, but persistence of hypokinesis in an area of previous regional wall motion abnormalities (RWMA). Concomitant EKG showed deep T-wave inversion in precordial leads (EKG 2week) (Figure 2B). She was discharged 2 weeks later, with residual motor weakness. At follow-up 4 weeks after discharge, we performed TTE and EKG. Cardiac systolic function including RWMA normalized, but LV wall thickness was slightly increased on TTE (from baseline 6 mm to 15 mm maximum at apex) and EKG revealed persistent deep Twave inversions (TWI) in precordial leads (Figure 2C). After 12 weeks, the EKG showed sinus rhythm and resolution of TWI (Figure 2D).
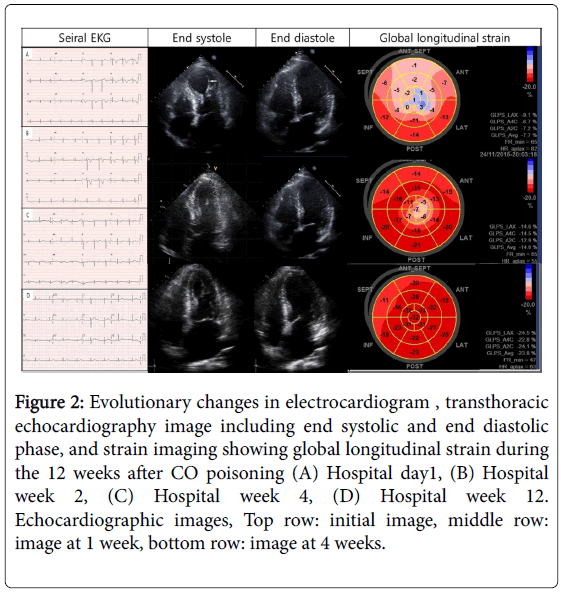
Figure 2: Evolutionary changes in electrocardiogram , transthoracic echocardiography image including end systolic and end diastolic phase, and strain imaging showing global longitudinal strain during the 12 weeks after CO poisoning (A) Hospital day1, (B) Hospital week 2, (C) Hospital week 4, (D) Hospital week 12. Echocardiographic images, Top row: initial image, middle row: image at 1 week, bottom row: image at 4 weeks.
According to Anderson et al, reversible cardiac failure may occur when the COHb level is greater than 25% [3]. Previous reports have shown that the recovery time from CO-induced CMP varied from 4 days to 6 weeks [4]. In the same study, however, most patients with CO-induced CMP, excluding those who died in the emergency room, recovered within 12 days after admission [5]. In the course of sCMP, there is a general clinical impression that almost full recovery occurs within 1-2 weeks, with normalized LV ejection fraction [6]. In some case reports, apical hypertrophy of the left ventricle was observed when wall motion had improved [7]. In some cases of sCMP, RWMA of the LV normalized and symptoms resolved 1 week after the acute phase. Interestingly, despite resolution of LV dysfunction, the LV apex in our patient showed a slight increase in wall thickness on follow-up in association with TWI in precordial leads on EKG, mimicking apical hypertrophic cardiomyopathy, with complete resolution in 1 month despite of delayed recovery of EKG change.
Our case showed normalization of RWMA and LV systolic function within 4 weeks of the index event, but recovery of TWI was delayed for 8 weeks after the index event in the precordial leads. Thus, normalization on serial EKG change was delayed, similar to that observed during the course of sCMP; this delayed recovery mimicked apical hypertrophy, with late recovery of RWMA and LV systolic function, unlike the in the course usually observed in cases of CMP induced by CO poisoning. In the future, for the better understanding of clinical course in CO poisoning sCMP, I suggested that prospective cohort study or registry study should be needed. In addition, multimodality imaging study including cardiac magnetic resonance (CMR) like previous study would be hepful for clinical characteristics of CO poisoning induced sCMP [7].
This study was case study and there were some limitations. We did not take an exam for screening for pheochromocytoma and for the better understanding for myocardial change in our case, we should have the test of CMR because of insurance and economic issues.
“In the future, for the better understanding of clinical course in CO poisoning sCMP, collaboration study with neurology division and combined study for treatment effect of high pressure oxygen should be needed. And serial echocardiographic studies including new technology for suttle change of myocardium such as strain analysis would be helpful for complementary study to CMR study.”
Among CO poisoning effects on heart, we experience a case of stress-induced cardiomyopathy (Scmp), with serial changes in EKGs and TTEs but delayed evolution of EKG recovery caused by CO poisoning. Further prospective studies for CO poisoning induced sCMP should be needed.