Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2013) Volume 2, Issue 2
Ectopic thyroid is an embryological abnormality resulting from the aberrance or failure of thyroid gland descent. We present a case of triple ectopic thyroid in a 10-year-old girl. Plain computed tomography and Tc-99m scans showed three ectopic thyroids located near the hyoid bone with no normally positioned thyroid. The patient was euthyroid at presentation, but hypothyroidism was observed five months later. On treatment with levothyroxine (75 μg/day), FT4 and TSH returned to normal ranges. Cases of multiple ectopic thyroidare are rare, with the present case being only the third case of triple ectopic thyroid presented. A careful follow-up is required because the incidence of malignancies associated with ectopic thyroid can be as high as 10%. Surgical treatment should be considered when the patient shows symptoms such as dysphagia, dysphonia, bleeding or dyspnea.
<Keywords: Multiple Thyroid Ectopy; Malignancy
A 10-year-old girl was admitted with a 1-month history of neck swelling. The lesion was a 20 mm × 15 mm soft, movable mass in the midline of the neck (Figure 1). Ultra sonography showed a solid midline mass, and plain computed tomography (CT) scans demonstrated three high-density masses around the hyoid bone near the base of tongue, pre hyoid region and pre-tracheal region, respectively (Figure 2). No normally positioned thyroid gland was observed. Laryngeal fiber scopic examination revealed a mass with a smooth surface at the base of tongue (Figure 3). The patient did not present with any airway obstruction or dysphagia. Tc-99m scans showed uptake in the region of the three masses. No uptake was seen in the normal thyroid (pretracheal) position (Figure 4). Serum FT3, FT4 and thyroid-stimulating hormone (TSH) levels were within normal ranges at presentation, although the thyroglobulin (Tg) level was elevated (218.7 μIU/L), and other laboratory tests were also within normal limits. Decreased FT4 (0.7 ng/dl), increased TSH (5.71 μIU/L) and further increased Tg (376.2 μg/L) levels were observed five months after the initial examination. The patients had screening test for congenital hypothyroidism and the abnormality was not pointed out. The patients have no the mental disability. A thyrotropin-releasing hormone (TRH) stimulation test was performed to evaluate the function of the pituitary gland.TSH level peaked 15 minutes after an intravenous bolus of TRH with the result within normal limits (Table 1). Although the reason why the patient became slightly hypothyroidism within five months was unknown, we decided to give levothyroxine to the patient because the swell of the ectopic thyroid and Tg elevation might be compensatory reaction for hypothyroidism. Treatment with levothyroxine (75 μg/day) resulted in FT4 and TSH levels returning to normal ranges together with a gradual decrease in Tg level.
| Time(min) | 0 | 15 | 30 | 60 | 90 | 120 |
| TSH(µIU/ml) | 2.8 | 29.9 | 25.1 | 15.1 | 9.1 | 5.6 |
Table 1: TSH values after stimulation by TRH.
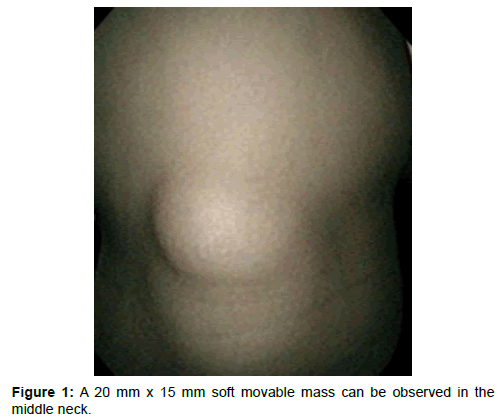
Figure 1: A 20 mm x 15 mm soft movable mass can be observed in the middle neck.
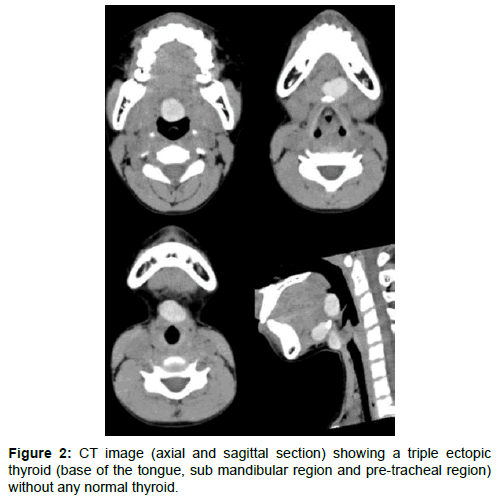
Figure 2: CT image (axial and sagittal section) showing a triple ectopic thyroid (base of the tongue, sub mandibular region and pre-tracheal region) without any normal thyroid.
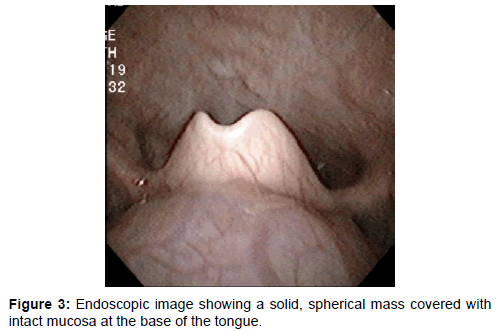
Figure 3: Endoscopic image showing a solid, spherical mass covered with intact mucosa at the base of the tongue
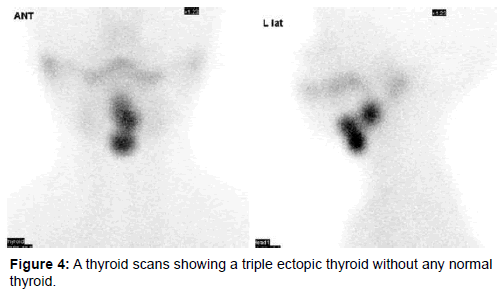
Figure 4: A thyroid scans showing a triple ectopic thyroid without any normal thyroid.
Ectopic thyroid, which was first reported in 1869 by Hickman, is an embryological abnormality [1]. The thyroid gland descends from the foramen caecum of the tongue to its final pre-tracheal position through the thyroglossal duct by 7 weeks gestation [2]. Ectopic thyroid arises from an aberrance or failure of its descent. Ectopic thyroid tissue usually occurs between the foramen caecum and the mediastinum.
Lingual thyroid (ectopic thyroid occurring at the base of tongue) is the most common type, accounting for 90% of all ectopic thyroids [3]. Other sites, all rare, include under the tongue, above the hyoid bone, in front of the larynx, the mediastinum, duodenum, esophagus, lungs and so on. A few cases of dual ectopic thyroid have been reported [4-5]. In most dual thyroid cases; the lesion is lingual and subhyoid. Only two cases of triple ectopic thyroid have been reported [6-7], with the present case being the third case.
The prevalence of ectopic thyroid varies between 1:100000 and 1:300000 and its clinical incidence is reported to range from 1:4000 to 1:10000.A male to female ratio of 1:4 is documented [8]. In 25% of cases, orthotropic thyroid tissue is also observed at the normal pretracheal position [2].
Most patients with ectopic thyroid are asymptomatic [9]; however, symptoms such as dysphagia, dysphonia, bleeding or dyspnea may occur as the ectopic thyroid (especially in cases of lingual thyroid) grows [10-11]. Thyroid function is either hypothyroid or euthyroid in most cases. About 33-62% of the patients with ectopic thyroid showed hypothyroidism with increased levels of TSH [12].A few cases of hyperthyroid have also been reported [13].
Thyroid scanning using technetium Tc-99m is the most useful tool for definitive diagnosis [8]. Thyroid scanning detects the presence of thyroid tissue in other sites. Additional CT scans or MRI may help in defining the extent or location of the ectopic thyroid gland. Differential diagnosis includes angioma, adenoma, fibroma, lipoma, lymphangioma and cysts in the neck [8], with thyroglossal duct cysts, which arise from epithelial remnants of the thyroglossal duct, also representing a major differential diagnosis. Thyroglossal duct cysts present as low-density masses on plain CT, whereas ectopic thyroid shows a high density as in our case [7].
Management of ectopic thyroid is controversial. If the patient is both asymptomatic and euthyroid, no treatment is required. The main concern is the risk of thyroid carcinomas, in most cases papillary carcinomas [14], arising from the ectopic thyroid tissue. Jarvis et al. reported that the risk of malignancies in cases of ectopic thyroid was 1% in 1969 [15]. This figure was quoted from a review published in 1934. Massine et al. reviewed 28 case reports of lingual thyroid carcinoma [16] and, in review of the English literature, we found that 33 cases of ectopic thyroid carcinoma has been reported in approximately 400 cases of ectopic thyroid (Table 2). This indicates that the potential for malignancy is as high as 10%. The reason for the very high incidence malignancy (10%) in ectopic thyroid tissue that we found in the literature is unknown. One possible reason is that ectopic thyroid tissue only calls medical attention when there is an enlargement due to infection, tumors etc. Asymptomatic lingual thyroid glands were found in as much as 10% of the autopsies. Therefore, ectopic thyroid glands are probably much more common than it is reported. In this sense the rate malignancy may be probably much lower than 10%. Even though, careful follow-up for cases of ectopic thyroid is necessary. In our case, fine needle aspiration cytology would be needed when the ectopic gland has more enlarged.
| Case no | Author | Date | Pathology | |
|---|---|---|---|---|
| 1 | Stith JA | 1981 | Papillary adenocarcinoma | |
| 2 | Laing MR | 1988 | Mixed papillary-follicular carcinoma | |
| 3 | Michigishi T | 1991 | Papillary carcinoma | |
| 4 | Zink A | 1991 | Papillary carcinoma | |
| 5 | Satta MA | 1991 | Papillary carcinoma | |
| 6 | Hoffmann R | 1991 | Papillary carcinoma | |
| 7 | Betkowski A | 1993 | Follicular carcinoma | |
| 8 | Cervera-Paz FJ | 1994 | Papillary carcinoma | |
| 9 | Jayaram G | 1995 | Papillary carcinoma | |
| 10 | Sand J | 1996 | Papillary carcinoma | |
| 11 | Subramony C | 1997 | Follicular carcinoma | |
| 12 | Hirnle T | 1997 | Follicular carcinoma | |
| 13 | See AC | 1998 | unknown | |
| 14 | Tucci G | 1999 | Follicular carcinoma | |
| 15 | Casella A | 1999 | Papillary carcinoma | |
| 16 | Hari CK | 1999 | Tall cell variant of papillary carcinoma | |
| 17 | Massine RE | 2001 | Papillary carcinoma | |
| 18 | Kao SY | 2002 | Papillary carcinoma | |
| 19 | Pérez JS | 2003 | Papillary carcinoma | |
| 20 | Ling L | 2004 | Papillary carcinoma | |
| 21 | Lee HY | 2004 | Papillary carcinoma | |
| 22 | Miller RS | 2005 | Papillary carcinoma | |
| 23 | Ling L | 2005 | Follicular variant of papillary carcinoma | |
| 24 | Shah BC | 2007 | Follicular variant of papillary carcinoma | |
| 25 | Yaday S | 2008 | Medullary carcinoma | |
| 26 | Choi JY | 2008 | Metastatic papillary thyroid carcinoma | |
| 27 | Kandogan T | 2008 | Follicular variant of papillary carcinoma | |
| 28 | Hari CK | 2009 | Follicular variant of papillary carcinoma | |
| 29 | Adotey JM | 2009 | Papillary adenocarcinoma | |
| 30 | Cordes S | 2010 | Papillary carcinoma | |
| 31 | Sevinç AI | 2010 | Papillary carcinoma | |
| 32 | Wang YJ | 2010 | Papillary carcinoma | |
| 33 | Borges A | 2010 | Papillary thyroid microcarcinoma | |
Table 2: Reported cases of carcinomas arising from ectopic thyroid.
It should be also kept in mind that, even if the patient is euthyroid, the patient could later develop hypothyroidism as in our case. If the patient is hypothyroid with an elevated TSH, thyroid hormone therapy might prevent enlargement or malignant transformation of the ectopic thyroid [9,17]. Surgical treatment should be considered when the patient is symptomatic [18]. Also, cervical ectopic thyroids may be removed surgically for cosmetic reasons. Several external or trans-oral surgical approaches have been described [19].