Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2012) Volume 1, Issue 1
Tuberculosis of thyroid gland is a very rare condition even though the incidence of extra pulmonary forms of tuberculosis is increasing. According to literature, frequency of thyroid tuberculosis is 0.1%–0.4%. We report a case of 66year old female patient with primary tuberculosis of thyroid gland. The diagnosis was established on histopathological examination after surgery. Patient underwent combination treatment with anti-tubercular chemotherapy
<Keywords: Thyroid; Tuberculosis
Tuberculosis of thyroid is extremely a rare clinical entity. A very few cases are reported from India, despite a high incidence of tuberculosis. The tuberculous involvement of thyroid gland is so rare that according to Rokitansky (1859) it never occurs. Clute and Smith (1927) reported one case of thyroid tuberculosis in approximately 1200 thyroidectomies and Levitt (1959) recorded only 2 cases among 2114 operations on thyroid gland [1]. Rankin and Graham found thyroid gland tuberculosis in 21 of 20758 (0.1%) cases of thyroid gland excision. There are approximately 200 cases of tuberculosis of thyroid reported throughout medical literature [2]. Recently we came across a case of Tuberculosis of thyroid.
We present a 66 year old female patient, who presented with complaints of progressive, painless swelling over right side of neck since 1 year (Figure 1). Patient had history of significant weight loss, heat intolerance and excessive sweating. Clinically there was solitary nodule of right lobe of thyroid, non-tender, soft in consistency, with welldefined borders with right jugulo-digastric lymphadenopathy. The rest of oral cavity and oro- pharyngeal examination was unremarkable. The systemic examination was also unremarkable. Fine needle aspiration cytology (FNAC) of thyroid nodule - reported as follicular neoplasm and from the cervical lymph nodes as nonspecific lymphadenitis. The haematological, thyroid profile and chest radiograph was normal except for elevated Erythrocyte Sedimentation rate (ESR). X-ray of neck was normal. Ultrasound of thyroid showed right sided hypo echoic nodule with minimal peripheral vascularity. Liver function tests were within normal limits. Tuberculin test was negative.

Figure 1: Patient with thyroid swelling.
Patient underwent right hemithyroidectomy with preservation of parathyroids and excision biopsy of lymph nodes. Histopathology report of specimen was suggestive of follicular adenoma with tuberculous thyroiditis (Figure 2 and Figure 3), and surprisingly, lymph nodes were negative for tuberculosis. Patient had uneventful postoperative course except for seroma, which was treated by aspiration. She was started on anti-tubercular chemotherapy for 6 months. Follow up showed, no signs or symptoms of localized or systemic tuberculosis.
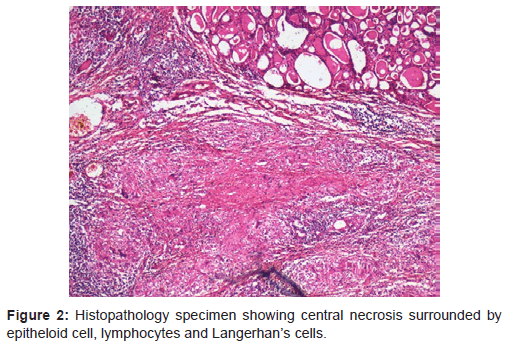
Figure 2: Histopathology specimen showing central necrosis surrounded by epitheloid cell, lymphocytes and Langerhan’s cells.
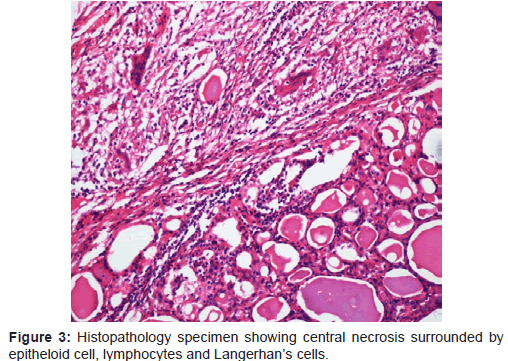
Figure 3: Histopathology specimen showing central necrosis surrounded by epitheloid cell, lymphocytes and Langerhan’s cells.
Tuberculosis of thyroid gland is rare. The hypothesis for this rarity in thyroid include: (i) Colloid material possessing bactericidal action (ii) Extremely high blood flow and an excess of iodine (iii) enhanced destruction of bacilli by increased activity of phagocytes in hyperthyroidism [3].
Tuberculosis of thyroid is usually unsuspected because of its rare occurrence, except in patients who already have tuberculosis of another organ , furthermore it is manifested with wide array of nonspecific symptoms like evening rise of temperature, weight loss, malaise ,night sweating, or even be asymptomatic [4]. Tuberculosis of thyroid is difficult to distinguish from other inflammations of thyroid as well as from carcinoma of thyroid because regional lymphatic nodes were also infiltrated. It is particularly vital to distinguish thyroid tuberculosis from thyroid cancer in order to avoid unnecessary surgery. In such cases, suspicion tuberculosis of thyroid gland should be made, if there is high Erythrocyte sedimentation rate (ESR), and positive tuberculin test. It is important to differentiate tuberculosis from other granulomatous diseases like De Quervain thyroiditis and Sarcoidosis [5].
In thyroid, tuberculosis may present as localized swellingmimicking carcinoma or cold abscess, or multinodular goite, or rarely as acute abscess. Thyroid tuberculosis can also manifest itself as thyroid nodule or lump or as nodule with cystic component [5]. The clinical presentation is often sub acute, or even patient be asymptomatic [6].
Past history of tuberculosis concomitant with cervical lymphadenopathy and sites of tuberculous involvement might lead to the correct clinical diagnosis. If mycobacterial infection is suspected, chest X ray and tuberculin skin test should be performed. Diagnosis is made only after Fine needle aspiration cytology or after histopathological examination of surgical specimen when Fine needle aspiration cytology is negative [6]. Characteristic findings include epithelioid cell granulomas with central caseous necrosis, peripheral lymphocytic infiltration, and Langhan’s giant cells [7]. Caseous necrosis is cytologic finding specific to tuberculosis. Simultaneous demonstration of acid fast bacilli (AFB) is diagnostic. In these situations mycobacterial culture is helpful [8]. Thyroid function is preserved in majority cases. Polymerase chain reaction (PCR) for mycobacterium tuberculosis is reliable diagnostic tool and if available, should be performed.
Imaging techniques are not very helpful in establishing diagnosis and been described only sporadically due disease’s rare occurrence. Ultrasonography usually reveals heterogenous, hypoechoic mass similar to neoplastic lesion. Contrast-enhanced Computed tomography may help to localize caseous lesion. Recent study has been done which has described Magnetic Resonance Imaging (MRI) features of thyroid tuberculosis, shows intermediate signal intensity due to presence of densely cellular inflammatory granulation tissue, with tuberculous granulomas with or without minimal necrosis [9]. However, this appearance in thyroid is nonspecific, and thyroid carcinoma shows similar feature.
Differential diagnosis depends on presence or absence of local pain. If pain is predominant clinical finding, differential diagnosis lies between infectious form and sub-acute granulomatous thyroiditis .Many diseases cause granulomatous inflammation, like granulomatous thyroiditis, fungal infection, tuberculosis, sarcoidosis, granulomatous vasculitis, and foreign body reaction. However, caseation necrosis is seen only in tuberculosis [10]. Tuberculosis should be considered in the list of differential diagnoses for thyroid abscesses and nodular lesions in people living in geographic regions with high tuberculosis prevalence [11].
Initially, treatment of thyroid tuberculosis consisted of antituberculous drugs combined with surgical removal of affected parts of thyroid or surgical drainage [12]. Now, it has been recognized that complete resolution usually follows an appropriate antituberculous chemotherapy only [12].
Although rare, Tuberculosis of thyroid gland should be included in differential diagnosis of thyroid swellings especially in countries like India, where there is high prevalence of tuberculosis. Fine needle aspiration cytology, Acid Fast bacilli (AFB) staining, culture of the aspirate and Polymerase Chain Reaction is important diagnostic tools in these cases. Antituberculous therapy is itself effective, in these forms of tuberculosis.