Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2013) Volume 2, Issue 3
A patient with myotonic dystrophy and associated multinodular goiter, subclinical hyperthyroidism, and follicular thyroid cancer is described. To authors’ knowledge, at least 12 cases of thyroid cancer associated with myotonic dystrophy have been reported which were papillary, medullary, and unknown type. This is the first reported case of follicular thyroid cancer in type 2 myotonic dystrophy. Myotonic dystrophy commonly involved endocrine system and unstable neucleotide repeat expansions in myotonic dystrophy may predispose patients to develop cancer. The authors hypothesized that myotonic dystrophy might be one of risk factors for development of thyroid cancer.
<Keywords: Myotonic dystrophy; Thyroid cancer
Myotonic muscular dystrophy (MMD) is an autosomal-dominant, multisystem disorder, and is one of the most complex disorders known. It comprises 2 subtypes. Myotonic dystrophy type 1 results from an expanded CTG repeat in a protein kinase gene on chromosome 19 [1]; in type 2, the defect is a CCTG repeat expansion in the gene for zincfinger protein-9 on chromosome 3 [2]. MMD is the most common adult muscle dystrophy, with an estimated prevalence of 1 in 8000 [3]. The disease is characterized by muscle weakness, dystrophic changes in neuromuscular tissues, frontal baldness, premature cataracts, cardiac disturbances, and intellectual impairment. The endocrine system is commonly involved, including primary testicular failure, insulin resistance, and various thyroid diseases. Several studies on cancer risk suggested that patients with myotonic dystrophy are at increased risk of developing various type of cancer [4,5].
There have been case reports of myotonic dystrophy associated with abnormal thyroid function [6-11] and goiters [12,13]. On very rare occasions, cases of thyroid neoplasm (three papillary, three medullary, six unknown type) associated with myotonic dystrophy has been reported in literature [4,5,14-16].
In this article, we describe first reported case of male with type 2 myotonic dystrophy associated with three thyroid abnormalities; multinodular goiter, subclinical hyperthyroidism, and follicular thyroid cancer.
A 64 year old male (Figure 1) with past medical history of muscle weakness, hyperlipidemia, constipation, and depression presents in a wheelchair for fine needle aspiration of a thyroid nodule. Patient first noticed to have muscle weakness 20 years ago when he was unable to release grip from hand shake and had difficulty holding a glass. The weakness was gradually progressive in arms and legs and eventually patient became wheelchair bound for the past 8 years. In 1987, patient became severely hypotensive and had complete heart block which require placement of pacemaker. Patient has bilateral cataracts, proximal muscle weakness, requires nightly oxygen therapy. Patient has no history of smoking or drinking. Patient completed high school and 2 years of college before he ran out of funds. Subsequently he worked selling open stocks in the foreign stock exchange. Patient was married in 1975 and marriage was dissolved after 3 years due to difficulty in maintaining sexual relations. Patient lives home alone with home attendant available 24 hours a day. Patient’s mother died of Multiple Sclerosis in 1999 at age 76. Patient’s father died of myocardial infarction at age of 68.
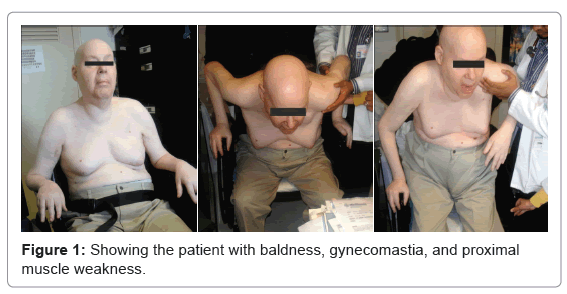
Figure 1: Showing the patient with baldness, gynecomastia, and proximal muscle weakness.
On physical examination he was well nourished, in no distress, bald, missing lateral portion of both eyebrows, and diminished facial macules. Thyroid gland was enlarged, estimated 300 g with multiple nodules. The largest nodule 6.5×4.5 cm in RT lobe hard in consistency non tender, no substernal extension, no bruits no palpable lymph nodes. Examination of chest revealed presence of a pacemaker. Significant bilateral gynecomastia, Muscle atrophy present bilaterally in both hands and legs, strength inadequately bilaterally in both upper and lower extremities. Positive movement restriction in standing from sitting position, negative joint crepitus, negative deformity. Normal sized testicles were noted. Neurological exam was positive for ptosis, gait disturbance and weakness.
Thyroid sonogram revealed a multinodular goiter, with a 6.5×5×4.5 cm solid nodule in right lobe and 1.2×1.1 ×1.2 and 1.3×1.1×1.1 cm in the left lobe. Laboratory tests were significant for thyroid stimulating hormone 0.19 (0.34-5.6) mIU/mL, triiodothyronine 77.8 (87-178) ng/ dL, thyroxine 8.12 (6.09-12.2) mcg/dL, anti TPO antibodies negative, free thyroxine 0.87 (0.58-1.64) ng/dL, testosterone 184 (212-755) ng/dL, prolactin 16.57 ( 1-20 in male) ng/mL, follicle-stimulating hormone 24.12 (<22 in male) IU/L, luteinizing hormone 26.42 (7-24 in male) IU/L. Fine needle aspiration of this nodule revealed follicular lesion. Due to large nodule the patient underwent total thyroidectomy and central neck dissection with removal of eight lymph nodes were done. All Lymph node were negative for metastasis. Pathologic examination of the tumor revealed a 5.2×4.3×3.6 cm tumor located in the middle area of right lobe of the thyroid; microscopically uniform microfollicular architecture of epithelial cells lining the follicles with no evidence for psammoma bodies and no nuclear changes, margins involved by carcinoma invasion of the capsule, with extra thyroidal extension. Also 3 vascular invasion were identified (Figures 2a and 2b), peripheral invasion was not identified. Pathologic staging: Stage II B [T3 CN0PN0M0]. After surgery patient received 100 mCi I131 ablation therapy, while TSH was 45 mIU/mL, and thyroglubin was 4.6 ng/mL. Post therapy scan revealed 1.2% uptake in thyroid bed, no evidence for distant metastasis. Patient was put on levothyroxine suppression therapy. Unfortunately, nine weeks post surgery, before getting repeat thyroid function and thyroglobulin level while on levothyroxine suppression therapy, he passed away at home after chocking a piece of meat.
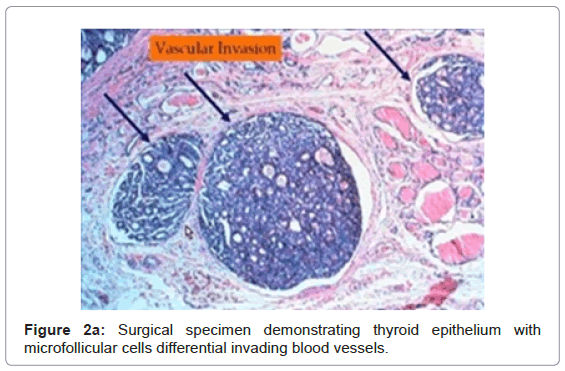
Figure 2a: Surgical specimen demonstrating thyroid epithelium with microfollicular cells differential invading blood vessels.
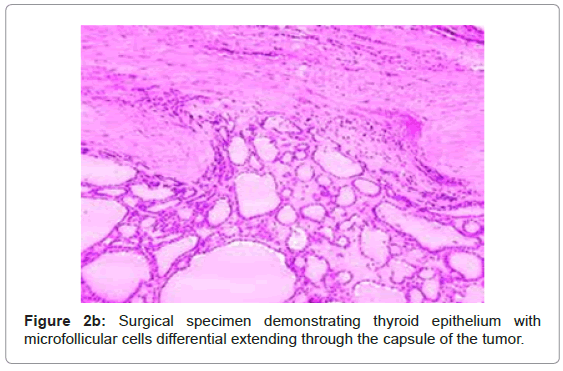
Figure 2b: Surgical specimen demonstrating thyroid epithelium with microfollicular cells differential extending through the capsule of the tumor.
This patient had clinical features of myotonic dystrophy type 2. His laboratory tests were consistent with gonadal failure and thyroid function tests revealed subclinical hyperthyroidism. He also had a multinodular goiter harboring follicular thyroid cancer.
A few cases of myotonic dystrophy associated with hyperthyroidism [8,11,17-19] or hypothyroidism [7,10,12,20] have been described, and two cases associated with non toxic multinodular goiter [12,13]. Our patient is the first reported case of myotonic dystrophy associated with multinodular goiter, subclinical hyperthyroidism, and follicular thyroid cancer.
It is known that type 1 myotonic dystrophy is caused by unstable trinucleotide (CTG) repeat expansion of the dystrophia myotonicaprotein kinase (DMPK) gene. Daumerie et al. [21] studied the CTG tripet expansion in a patient with type 1 myotonic dystrophy associated thyroid nodular disease and reported that 7 times larger amplification was found in abnormal thyroid tissue compared to lymphocytes, suggesting that anomalies in the DMPK gene might contribute to thyroid dysfunction [21]. However, there is no similar study conducted on type 2 myotonic dystrophy.
As both myotonic dystrophy type 1 and type 2 result from unstable neucleotide repeat expansions in their respective genes. This underlying genetic instability may predispose these patients to developing tumors [22]. There have been multiple reports of tumors in individuals with myotonic dystrophy, most commonly benign, calcifying cutaneous tumors knows as pilomatricomas [13]. In addition to pilomatricomas, a variety of benign and malignant neoplasm has been described in myotonic dystrophy type 1 and type 2 [22] (Table 1).
| Type of Tumor | Number of cases | Type of Tumor | Number of cases | |
|---|---|---|---|---|
| Thyroid Carcinomaa | 12 | Other GI track | 6 | |
| Thyroid Adenoma | 1 | Lung | 13 | |
| Thyroid Goiter | 2 | Breast | 16 | |
| Non melanoma skin cancer | 14 | Endometrium | 12 | |
| Melanoma | 11 | Ovary | 9 | |
| Pituitary | 2 | Other female genital organ | 3 | |
| Parathyroid | 9 | Prostate | 11 | |
| Insulinoma | 2 | Testis | 4 | |
| Pheochromocytoma | 1 | Kidney | 5 | |
| Thymoma | 9 | Other urinary organs | 2 | |
| Colorectum | 19 | Brain | 8 | |
| Liver | 2 | Leukemia | 4 | |
| Pancreas | 4 | Lymphoma | 8 | |
| Parotid gland | 5 | Other sites | 11 | |
| Total | 205 | |||
Table 1: Summary of type of tumor and number of cases in literature in patients with myotonic dystrophy type 1 and type 2, aTwelve cases were 3 medullary carcinoma, 3 papillary, and 6 unspecified.
There have been 2 studies done in purpose to quantified cancer risks in patients with myotonic dystrophy [4,5]. Win et al. [5] reported an increase risk of thyroid cancer and choroidal melanoma based on 307 patients with myotonic dystrophy type 1 and type 2 from Mayo Clinic, Rochester, MN. They observed an approximately 6-fold increased risk of thyroid cancer compared with general population. However, Gadalla et al. [4] conducted larger multinational study including 1658 myotonic dystrophy patients from Swedish and Danish Registry and reported result differently. Their study identified significant increased risks for cancers of the endometrium, brain, ovary, and colon. Although the study suggested possible excess of thyroid cancer with Standardized Incidence Ratios of Cancers of 7.1 and P value of 0.01, the authors aimed to focus primarily on associations with P values less than 0.01 to minimize testing-related false discovery.
Our reported case has three different abnormalities in thyroid gland including multinodular goiter, subclinical hyperthyroidism, and the first ever reported case of follicular thyroid cancer in type 2 myotonic dystrophy.
Till now an association between myotonic dystrophy and thyroid cancer remains unclear. The neoplasms of thyroid associated with myotonic dystrophy that have been reported are: one adenoma, two goiters, and twelve thyroid carcinoma (three papillary, three medullary, six unknown type). Our patient is the first case report of follicular thyroid cancer associated with type 2 myotonic dystrophy. Further research is needed to definitively address an association between myotonic dystrophy and thyroid cancer and to understand the biological mechanism. If this is a strong association, myotonic dystrophy should be added as a risk factor for development of thyroid cancer.