Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Short Communication - (2014) Volume 4, Issue 3
Clinical trial dropout is a major obstacle to understanding the most effective depression treatments for low-income, minority depressed cancer patients. This study reports provider perspectives of barriers in a cohort of low-income, predominately minority cancer participants who were enrolled and then dropped out of a large NCI-funded depression treatment trial (Alleviating Depression among Patients with Cancer [ADAPt-C]); and uses Andersen and Newman’s Individual Determinants of Health Service Utilization (2005) model as a socio-culturally sensitive framework to explore retention priorities among underserved cancer patients in depression treatment. This was a qualitative study conducted from a subset of 15 ADAPt-C dropout participants. Provider clinical chart notes were abstracted to identify barriers to continuing treatment and a template analysis approach was used to identify general issues related to dropout. Providers reported: Predisposing component barriers related to patients’ Social Structure and Beliefs; Enabling barriers related to Family and Community; and Perceived Illness
barriers related to their Perceived and Evaluated Illness. This study illuminates newly identified predisposing “psychological coping” belief barriers. Findings reveal that the classic work of Andersen and Newman’s (2005) model of health use is a useful heuristic for categorizing retention barriers, distinguishing the family, and other societal, health services system, and individual factors. This knowledge will help develop interventions that address barriers among this population and will help develop better clinical trial recruitment and retention strategies to help hard-to-reach populations remain in treatment.
Keywords: Clinical trials; Low-income; Minority; Retention; Depression; Cancer
Depression treatment clinical trial dropout presents a significant obstacle in the retention of cancer patients to depression treatment clinical trials, as patients with cancer who are most in need of psychosocial interventions may be more likely to drop out [1,2]. This is especially critical given that cancer is the leading cause of death for racial and ethnic minorities [3] and low-income populations in the United States [4]. This burden is also alarming given the coexistence of cancer and depression being associated with significantly increased mortality [5-8]. Existing psychosocial intervention studies have been based almost exclusively on White populations [9,10], fail to describe the ethnic composition of the sample, completely omit discussion of ethnic minority sample description, were not conducted in public care systems, or provide little explanation of attrition problems [11-13].
Although much research has been conducted on the determinants of or factors related to adherence and retention in general, few studies have addressed clinical trial retention among cancer patients in depression treatment for a predominately low-income, minority population. Therefore, this study aims to report and describe provider perspectives of retention barriers in a cohort of low-income, predominately minority cancer participants who were enrolled and then dropped out of a large NCI-funded depression treatment trial, Alleviating Depression among Patients with Cancer (ADAPt-C) [14,15]. Using primary data from provider clinical documentation, this study also sheds light on retention priorities.
This qualitative study used document review methods. It was conducted from a subset of ADAPt-C [15] dropout participants, in which provider medical chart records were abstracted to identify a comprehensive list of psychosocial barriers and factors, which contributed to dropout, based on Andersen and Newman’s [16] model. The intervention is an individualized stepped care depression treatment program provided by a Cancer Depression Clinical Specialist (CDCS) in collaboration with a study psychiatrist. Patients randomized to the intervention are offered antidepressant medication and/or problem solving treatment, a cognitive–behavioral treatment, which has been found effective in treating depression among Latinos, particularly when socio-environmental stress is a significant factor [17-20].
In January and February 2008, ADAPt-C intervention dropout participants were recruited by telephone, and then were mailed the medical release consent. Those who did not respond by telephone, with at least eight attempts were mailed a written study invitation along with a self-addressed stamped envelope, requesting that they indicate a convenient time to call back to discuss participation and medical record release.
Two-hundred-forty-two patients were enrolled in the ADAPt-C depression treatment intervention, with 152 satisfying criteria of adhering to treatment. Of the 96 ADAPt-C study intervention participants who did not see a therapist at all or did not see the therapist after the first initial visits, 39 initially completed the ADAPt-C baseline assessment, and were randomized to the ADAPt-C intervention. Figure 1 shows the dropout recruitment, leaving 15 dropout patients in this study sample pool. Figure 2 represents the medical release form recruitment and retention details.
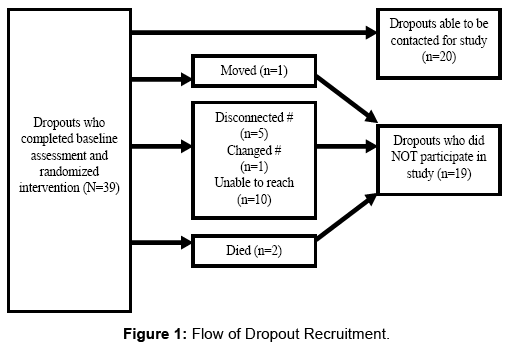
Figure 1: Flow of Dropout Recruitment.
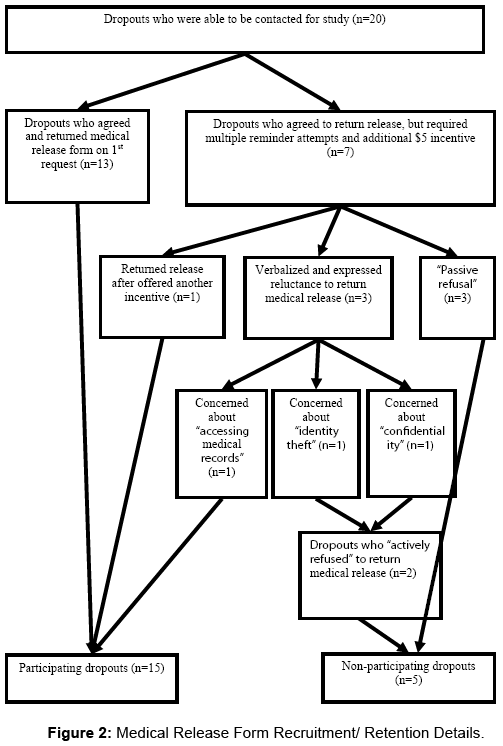
Figure 2: Medical Release Form Recruitment/ Retention Details.
A template analysis approach [21] was used to identify the general issues related to dropout, based on a priori sensitizing concepts from Andersen and Newman’s [16] variable categorization which focuses on: the individual to use services (Predisposing), the ability to secure services (Enabling), and the illness (Illness).
Table 1 reports the sample’s demographic characteristics: Predominately female, Latino, foreign-born, Spanish-speaking, in the U.S. for more than 10 years, and unemployed. These characteristics were similar to the overall ADAPt-C parent study characteristics.
| Demographic Characteristics | Participating dropouts (n = 15) | Non-participating dropouts (n = 5) |
|---|---|---|
| Female | 14 (93%) | 4 (80%) |
| Latino | 12 (2 African American, 1 White) (80%) | 5 (100%) |
| 50+ years old Foreign-born | 9 (60%) 11 (73%) | 4 (80%) 5 (100%) |
| Spanish-speaking | 11 (73%) | 5 (100%) |
| In US 10+ years | 12 (80%) | 4 (80%) |
| Unmarried | 7 (46%) | 4 (80%) |
| Unemployed | 14 (93%) | 3 (60%) |
| Education ≥ 12th grade | 10 (66%) | 2 (40%) |
Table 1: Demographic characteristics of participating and non-participating dropouts.
Figure 3 illustrates the provider explanatory model of dropout patient barriers based on the Andersen and Newman’s model [16] categorization. Providers reported Predisposing component barriers related to patients’ Social Structure (e.g., being unemployed and needing to seek work; work time conflicts [e.g., inability to leave work until 6pm or working 12 hour shifts]; caregiving demands (e.g., grandkids); “housing instability;” patient “moved” due to needing more affordable housing, which led to proximity problems; lack of social support/ isolates self (e.g., “no friends”); job stress, transportation problems; and Financial problems (e.g., due to no sick time); and “Psychological Coping” Beliefs (e.g., patient reportedly “feeling better,” patient “not interested,” “emotional stress,” grief over a “loss” (of 15 year old son), history of untreated panic attacks, and anxiety over desired pregnancy (i.e., need to prevent or delay pregnancy). Providers also reported two levels of Enabling component barriers related to the original Family and Community model levels. Provider-documented Family barriers included family financial problems, “conflict with family,” poor family communication, and family attitudes regarding cancer. Community level barriers included the change of medical and/or mental health providers in the community and patient dissatisfaction with hospital and medical services. Perceived Illness-level barriers included patient health concerns, “chemotherapy treatment” barriers, and the severity of the illness-related “pain.” Evaluated Illness-level barriers included their existing cancer diagnosis, depression or depressive symptoms, and other existing co-morbid illness (e.g., diabetes and hypertension).
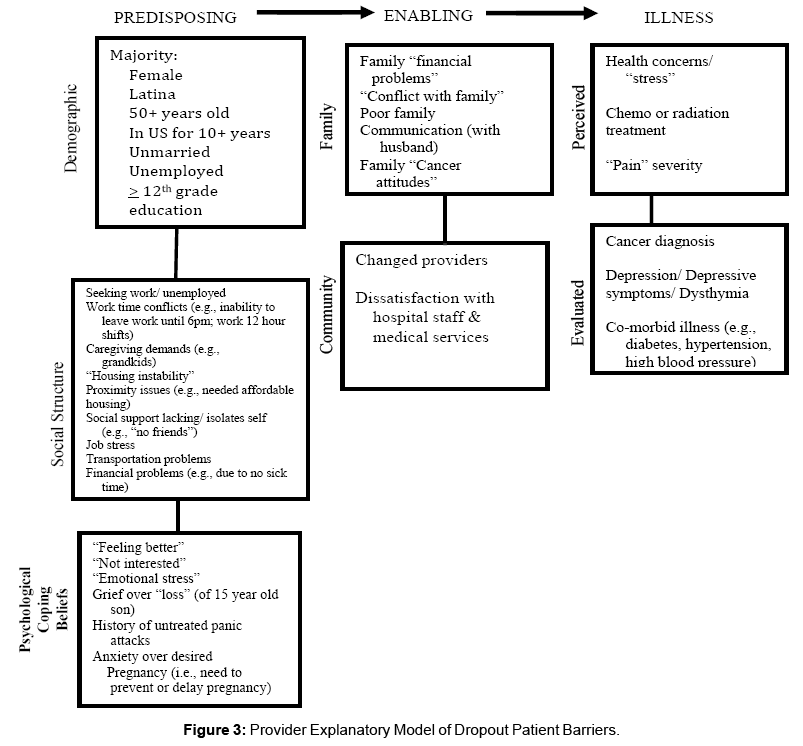
Figure 3: Provider Explanatory Model of Dropout Patient Barriers.
This study identifies many of the same barriers found in the literature that categorize Latino clinical trial retention barriers: familial relationships and issues [22], lack of transportation, employment interferences [23], economic stress [24] and financial costs [25], insufficient caregiving resources to meet demands [26], practical barriers [24,27], like interference with other top priorities of life such as work and family obligations[26], and systems barriers [28-30]. Andersen and Newman’s [16] framework helps illuminate new and important Predisposing “Psychological Coping” Belief barriers specific to this co-morbid population, that are not specifically indicated in the literature (i.e., “feeling better;” “not interested;” “emotional stress;” grief over “loss;” untreated panic attacks; and anxiety over fertility issues). However, there are also other possible relevant cultural barriers (i.e., distrust, fear, and language issues [26,31,32]) and provider barriers (i.e., inflexibility on the researchers’ part to reschedule, lack of feedback from the research team [26]) indicated in the literature which were not captured in this study’s medical record documentation. Such cultural and provider barriers are more sensitive issues that are less commonly explored and documented. This issue rises to clinical importance, given that providers might traditionally focus more on common practical barriers that are frequently identified, instead of acknowledging others. Documentation is a form of ethical accountability that requires the provider to indicate relevant barriers, even if they might be less common and somewhat more sensitive in nature. Ultimately, the purpose of documentation is to treat the patient better [33] which requires others to fully comprehend a full range of barriers and facilitators to participation and/or completion.
It is particularly interesting that some dropouts passively refused (n=3) to actually mail in the release, despite verbally agreeing to return it multiple times. This may reflect an element of just “pleasing” the provider (which may be influenced by cultural factors), or perhaps the interference of life priorities and demands got in the way of follow-through [26]. This might also be a matter of skepticism and reluctance over medical research or clinical trial research. It would also be interesting to find out if better rapport or a more established relationship between the recruiter and potential patient would have improved the likelihood of returning the release. With ethical human subject considerations, clinicians and researchers need to be cognizant of the desired types and value of incentives in clinical trials, especially when trying to recruit and retain hard-to-reach participants.
Despite the many strengths of this study and the lessons learned, the nature of a qualitative study design, with a small number of patient medical records from those who discontinued treatment, limits the depth and range of explanations for dropout barriers. There was no opportunity to probe barrier statements as we could have with interviewing providers, so there were assumptions about what providers meant when they documented in the notes. In addition, the richness of data may vary from one provider to the next and there may have been great variability in the quality and quantity of data due to lack of standardization of preparation of these notes among different providers. However, this study design was able to highlight barriers that might not have been so apparent in other types of survey or interview study designs, and offer clues to similar and additional barriers contributing to dropout and retention, which is critical for intervention development.
This study demonstrates that even participants who drop out of a trial can still be re-engaged in a research study. Although the real reason for successful re-engagement is somewhat unknown (i.e., increased incentives, more familiarity and better rapport with recruiter, “people pleasing,” little time and effort with completing medical release form), we do know that intentional strategies can be used to retain and move hard-to-reach individuals. It is first important to gain a full range of sociocultural, psychosocial, provider, and health system factors and barriers that influence dropout, from triangulated perspectives and sources like this. This knowledge will help in the development of better clinical trial recruitment and retention strategies, geared toward addressing barriers that get in the way of enrolling and helping hardto- reach populations remain in treatment.
I thank the following who helped with challenging recruitment and data collection efforts for this study: Sylvia Barker, Maria Hu-Cordova, and Yvonne Parades-Alexander.
This project was funded by grants from the American Cancer Society, doctoral oncology fellowship (DSW-06-219-01-SW): the NCI Minority Research Supplement (3 R01CA105269-S1) (PI: Kathleen Ell, DSW), and an NCI F31 dissertation fellowship (1 F31 CA132623).