Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2015) Volume 0, Issue 0
Background and Objectives: Recombinant factor VIIa (rFVIIa) is approved for treatment of inhibitors in hemophilia but has also been used for numerous off-label indications. Type of study: This study aims to validate a modified Biss scoring system in patients who received recombinant factor rFVIIa in Jeddah, Saudi Arabia. Materials and Methods: We included 70 patients who received rFVIIa for off-label indications over 12 months. Characteristics of survivor and non-survivor groups were compared including demographics, laboratory and clinical data. Using a modified Biss prognostic scoring system, based on the original scoring system used by Biss and Hanley, patients were divided into low (<1), intermediate (1-2) and high (≥3) score groups. Results: The mean age of patients was 46.1(±18.6) years. The most common off-label indications for rFVIIa treatment were to control bleeding associated with cardiac surgery (33%) and management of intracranial hemorrhage (18.8%). Forty three patients (61.6%) were at low risk, 20(28.6%) were at intermediate risk, and 7 (10%) were at high risk. Survivors were younger than non-survivors and less likely to have coagulopathy, or renal impairment at the time of treatment. The total prognostic score correlated to survival outcome (P ≤ 0.042); 73.2%, 22%, 4.9% of survivors had a low, intermediate and high score, respectively. Conclusions: Our results suggest that a modified Biss score could help predict survival of patients receiving rFVIIa. Prospective studies are needed to further validate the utility of this scoring system.
Keywords: Recombinant factor VIIa; Off-label use; Hemorrhage; Survival; Blood transfusion
Recombinant activated factor VII (rFVIIa; NovoSeven, Novo Nordisk A/S, Bagsværd, Denmark) was specifically developed for use in hemophilia A and hemophilia B patients with corresponding factor inhibitors [1]. The Food and Drug Administration (FDA) approved rFVIIa in the United States in 1999 for management of bleeding episodes in patients with congenital hemophilia A or B with inhibitors (auto-antibodies to coagulation factors VIII and IX). The label was subsequently expanded to include patients with acquired hemophilia, congenital factor VII deficiencies and inherited platelet disorders [1,2].
The coagulation cascade can be divided into 3 pathways; the intrinsic, extrinsic and common pathways. Factor VIIa binds to extravascular tissue factor (TF), upon exposure to form TF/FVIIa complex which initiates the extrinsic pathway and produces small amounts of thrombin [3]. This simultaneously activates FIX and FX and activates the intrinsic pathway which amplifies thrombin generation many folds [4]. Thrombin subsequently cleaves fibrinogen to fibrin and a fibrin clot is formed.
Mechanism of action of FVIIa is multifold and includes both TF-dependent and platelet-dependent pathways [5]. Upon binding to TF, FVIIa generates sufficient amounts of thrombin to activate platelets. At pharmacologic doses, rFVIIa directly activates factor X on the surface of activated platelets, resulting in a thrombin burst and acceleration of coagulation [6,7].
The efficacy of rFVIIa depends upon coagulation factors, platelet number and function as well as changes in body temperature and pH [8-10].
The interest in the use of rFVIIa in the setting of acute, life-threatening bleeding in non-hemophiliacs has increased recently. In the absence of evidence of the efficacy of rFVIIa treatment in these diverse patient populations, the need for a clinical prediction scoring has intensified [11]. Previously, Biss et al. developed a clinical scoring system based on presence of each of the following; coagulopathy, renal impairment, advanced age, transfusion of >10 units of PRBCs, hypothermia and obstetric indications [12]. In his study Biss concluded that utilization of this scoring system might help predict clinical outcomes of rFVIIa treatment. In this retrospective study, we assessed the correlation of a modified Biss scoring system to clinical outcomes in patients treated with rFVIIa at major teaching hospitals in Jeddah, Kingdom of Saudi Arabia.
Patient selection and data
We excluded pediatric patients as well as those who received rFVIIa for FDA-approved indications. Patient data were accessed through medical records after obtaining approval of the hospital ethics committee. All patients received rFVIIa for management of life threatening bleeding when blood component therapy, surgical interventions and less expensive homeostatic agents such as antifibrinolytic agents and DDAVP (desmopressin acetate (1-deamino-8-D-arginine vasopressin) had all failed.
We obtained rFVIIa indications, laboratory data, dosage, blood component usage, and clinical outcome from medical charts. Blood component requirements during the 24 hours preceding and the 24 hours immediately following rFVIIa administration, were noted. In the absence of local guidelines for the use of rFVIIa for management of severe hemorrhage, rFVIIa was administered at the discretion of the physician. An initial dose of 90-μg/ kg (single dose or 2 doses 3 h apart) was used.
Modified Biss prognostic scoring system was devised as shown in Table 1. Patients were stratified into risk groups according to the total score. Data on hypothermia from literature review are conflicting thus it was excluded from the modified score [10,13,14].
| Prognostic Factor | Score | |
| Coagulopathy: Any of the following |
Platelet count ≤50 ×109/L Fibrinogen ≤1·0 g/L Or PT/APTT ≥1·5× ULN |
+1 |
| Creatinine ≥ 120 μmol/l | +1 | |
| ≥ 10 units of red cell transfusion | +1 | |
| Age ≥ 60 years | +1 | |
| Obstetric indication | -1 | |
| Total score | Low risk (score ≤ 1) | Intermediate risk (> 1 but < 3) |
Table 1: Modified Biss prognostic scoring system. ULN: Upper Limit of Normal.
The prognostic score was created by a simple additive method of the following variables: coagulopathy, renal Impairment, elderly age more than 60 years, presence or absence of obstetric indication and total packed red cell transfusion.
Statistical analysis
All analyses were conducted using Statistical Package: IBM SPSS version 22. Frequency statistics were used to show descriptive statistics for mean, range and variations of the variables. A simple Descriptive Statistics was done to present variables through counts and percentages for categorical variables while mean, range and variations for the continuous variables. A P-value of < 0.05 was considered to be statistically significant.
This study used Paired t-test and Wilcoxon test to compare related variables with normal and non-normal distribution respectively. To establish the demographical relationship between categorical variables this study used Chi-Square test. Furthermore, to relate the difference of mean prognostic scores, a t-test and a One Way ANOVA test was used for two groups and more than two groups respectively. Normality was assumed using Levene’s test for Homogeneity of Variance. In case of unequal variance Welch t-test was used as an alternative for the Standard t-test and a Post-Hoc test LSD (Least Significant Difference) was used as an alternative for One-Way ANOVA.
A p-value <0.05 was a criteria to reject the null hypothesis. A Power Analysis was also conducted to avoid Type I error in statistics.
Seventy consecutive patients were identified over a period of 12 months. Descriptive statistics were used to describe the patient’s characteristics including, and pre-dose laboratory testing. Table 2 lists patient sex, off-label rFVIIa indication, and clinical outcome.
| Variable | Count N=70 | % | |
| Gender | Male | 33 | 47.1 |
| Female | 37 | 52.9 | |
| Survival | Alive | 40 | 58 |
| Dead | 29 | 42 | |
| Indication | ICH | 13 | 18.8 |
| PPH | 8 | 11.6 | |
| Cardiac surgery | 23 | 33.3 | |
| Bleeding varesis | 9 | 13 | |
| Malignancy | 5 | 7.2 | |
| Others | 3 | 4.3 | |
Table 2: Patient demographics, survival outcome and indications for rFVIIa use. ICH, intracranial hemorrhage; PPH, postpartum hemorrhage.
The most common off-label indications for rFVIIa were bleeding following cardiac surgery, intracranial hemorrhage (ICH), and postpartum hemorrhage (PPH). Other indications included gastrointestinal tract (GIT) bleeding due to uremia or liver disease, and malignancy. Table 3 shows laboratory data before rFVIIa infusion. At the time of administration, 19 patients (27%) were younger than 60 years, 26 patients (37%) had coagulopathy, 24 patients (34%) had renal impairment, and 8 patients (11%) received rFVIIa for the management of obstetric bleeding.
| Variables | Min | Max | Mean | SD |
| Age | 15 | 80 | 46.11 | 18.6 |
| HB | 3.9 | 15.1 | 7.38 | 2.08 |
| Platelets | 10 | 598 | 187.39 | 138.3 |
| INR | 1 | 12.5 | 1.82 | 1.84 |
| APTT | 1 | 150 | 54.65 | 32.44 |
| FIB | 11 | 745 | 321.57 | 198.51 |
| D-dimer | 104 | 3400 | 821.8 | 790.98 |
| Ggt | 5 | 411 | 58.61 | 76.21 |
| CK | 4 | 1650 | 393.67 | 406.54 |
| Troponin | 0 | 321 | 63.74 | 109.55 |
| Creatinine | 18.4 | 1370 | 175.89 | 218.6 |
Table 3: Laboratory investigations at the time of presentation. HB, hemoglobin; INR, International Normalization Ratio; APTT, activated partial thromboplastin time; FIB, fibrinogen; CK, creatinine kinase.
The overall survival rate was 58%. Table 4 shows comparison of “survivors” and “non-survivors” groups. Survivors were younger and were less likely to have coagulopathy and renal impairment at the time of administration. Survival correlated significantly to the prognostic score (P ≤ 0.042) (Figure 1).
| Survival | N | Mean | Std. Deviation | p-value | |
| Platelets (x109/L) | Alive | 38 | 203.37 | 150.9 | 0.254 |
| Dead | 27 | 163.11 | 119.8 | ||
| INR | Alive | 39 | 1.39 | 1.1 | 0.035* |
| Dead | 25 | 2.08 | 1.5 | ||
| APTT | Alive | 40 | 50.17 | 28.3 | 0.138 |
| (Seconds) | Dead | 27 | 62.22 | 37.4 | |
| FIB | Alive | 26 | 336.65 | 193.6 | 0.734 |
| (mg/dl) | Dead | 19 | 316.26 | 203.5 | |
| GGT | Alive | 33 | 32.27 | 27.7 | 0.009** |
| (IU/L) | Dead | 20 | 103.5 | 107.4 | |
| Creatinine | Alive | 33 | 106.3 | 79.9 | 0.013** |
| (μmol/L) | Dead | 24 | 276.16 | 302.6 |
Table 4: Comparison of laboratory investigations in survivors and non-survivors. Platelets count, INR, International Normalization Ratio; APTT, activated partial thromboplastin time; FIB, fibrinogen; GGT, gama glutamyl transferase and creatinine level. *Significant using Independent t-test p ≤ 0.05 level, **Significant using Welch’s ttest p ≤ 0.05 level.
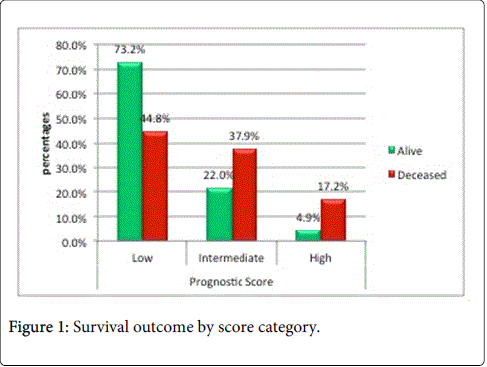
Figure 1: Survival outcome by score category.
Low-risk patients had a survival rate of 73%, intermediate-risk patients had a survival rate of 22% and high-risk patients had a survival rate of 4%.
Uncontrolled bleeding continues to be a major cause of mortality in cardiac surgery, post-PPH and ICH [15]. Consequently, rFVIIa is increasingly being used off-label as a „ generic hemostatic agent“. The off-label use of this medications is appealing when standard therapies prove ineffective [16]. A retrospective database analysis of off-label rFVIIa use in U.S. hospitals revealed that the off-label use of rFVIIa has increased more than 140-fold the majority of which were for off-label indications [17].
This series examines the use of rFVIIa as a haemostatic agent in the management of intractable hemorrhage. Table 5 shows the most common off-label uses of rFVIIa in our study. In this study, the most common off-label uses of rFVIIa were for cardiac surgery, ICH, and PPH, (33%, 18.8% and 11% respectively) which is comparable to that of other registries [18,19]. The majority of patients received a single dose (60%) and the mortality rate in this study is 58%, which is comparable to those seen in previous studies [12,20-22].
| Domains | Survival | p-value | ||
| Alive N=40 | Dead N=29 | |||
| Coagulopathy | No | 27(67.5%) | 16(55.2%) | 0.297 |
| Yes | 13(32.5%) | 13(44.8%) | ||
| Renal Impairment | No | 28(70.0%) | 17(58.6%) | 0.327 |
| Yes | 12(30.0%) | 12(41.4%) | ||
| Age ≥ 60 | No | 32(80.0%) | 18(62.1%) | 0.1 |
| Yes | 8(20.0%) | 11(37.9%) | ||
| Red Cell Transfusion | No | 35(87.5%) | 26(89.7%) | 0.072 |
| Yes | 5(12.5%) | 3(10.3%) | ||
| Obstetric Indication | Yes | 7(17.5%) | 1(3.4%) | 0.783 |
| No | 33(82.5%) | 28(96.6%) | ||
Table 5: Comparison of independent prognostic criteria in survivors and non-survivors. *Significant using Independent t-test; p ≤ 0.05 level, **Significant using Welch’s t-test p ≤ 0.05 level.
In coronary bypass surgery, national guidelines specify a transfusion threshold (e.g. 10 units of RBCs) that needs to be reached before rFVIIa should be given.
Refractory post cardiopulmonary bypass (CPB) hemorrhage is multifactorial and remains a major cause of mortality and morbidity [11]. In addition, ICH is one of the most serious subtypes of stroke [15]. There is good evidence from systematic reviews and randomized controlled trials that rFVIIa stops hemorrhage in adults with ICH if it is given within 4 hours of symptom onset [23]. Furthermore, few controlled clinical trials have demonstrated prolonged survival after the use of rFVIIa for the treatment of ICH; however, Yank V et al evaluated the efficacy of rFVIIa use for cardiac surgery and intracranial hemorrhage. He concluded that limited available evidence suggests no survival advantages for rFVIIa use [24]. Furthermore, case reports and case series suggest a potential benefit of rFVIIa in the management of severe PPH and upper gastrointestinal bleeding refractory to standard treatment [25,26].
Differences in patient characteristics are likely to have a major impact on survival. Application of the modified Biss scoring system to our population showed consistent predictability and highlighted important differences that may influence future criteria for patient eligibility to receive rFVIIa. Patients with a high score were less likely to survive and patients with low score were more likely to survive. These results are in line with the original study [12]. Survivors were younger age group and were less likely to have renal impairment reflecting lack of co morbidity. Impact on overall survival, with death resulting from multiorgan failure in the majority of non-survivors correlated to severity of co morbidities [12,21,27,28]. The improved survival in obstetric indications also reflects the relatively younger age and lack of pre-existing co morbidity [29,30].
Massive transfusion, accompanied by the development of dilutional coagulopathy frequently predicts mortality in patients with traumatic or surgical bleeding [31] our finding, that non-survivors also were more likely to have received a greater than 10-unit red cell transfusion which supports the theory that earlier treatment with rFVIIa improves outcome by preventing the complications of massive transfusion, dilutional coagulopathy and ongoing blood loss. Survivors were also less likely to have coagulopathy. The presence of severe coagulopathy at the time of rFVIIa administration has been shown in previous series to adversely influence outcome and overall survival [22,32] although this effect was not demonstrated in a larger study [21]. Data from the Hemostasis Registry have demonstrated that lower platelet counts are independently associated with mortality in patients treated with rFVIIa [17]. These conflicting reports highlight the advantage of using a prognostic score rather than a single prognostic indicator.
While some reports suggest the effect of hypothermia on coagulation enzymatic rates and platelet enzymatic and secretory rates, some studies failed to support these finding [10]. Viuff et al concluded that the efficacy of rFVIIa was affected by the degree of hemodilution and type of volume expander, but not by acidosis or hypothermia [10]. The ability of rFVIIa to enhance haemostatic parameters as evident from the improved TEG parameters at temperatures of 28-31°C in response to rFVIIa suggest that hypothermia is consistent with retention of enzymatic activity between 37 and 32°C in vitro and in vivo [33,34]. Furthermore, Hall et al did not find an independent relationship between transfusion requirement or repeat dosing and temperature following rFVIIa administration [9]. Therefore hypothermia was excluded from the modified Biss score.
Some randomized controlled trail of rFVIIa in trauma patients reported a trend toward reduced transfusion requirement and mortality [35]. A number of studies have described the development of off-license rFVIIa treatment guidelines in various clinical contexts [30,36-38]. Lack of randomized controlled trials results in practice guidelines based on weak recommendations, however, guidelines implementation improves patients outcome particularly when incorporating factors that are shown to influence outcome [39]. Furthermore, high levels of guideline compliance were evident whenever the number of possible elements in the scoring system is small. Therefore the use of a prognostic score may help to predict survival in patients appearing eligible for treatment with rFVIIa and may help to justify the use of this expensive medication associated with potential side effects.
Clinical practice guidelines are set to reduce costs without adversely affecting patient outcomes. In the absence of high-quality data, the absence of a laboratory test predicting response, and considering the high cost of rFVIIa, their concern about the off-label use of rFVIIa. The use of a clinical scoring system may help to predict outcome and may help allocating this expensive resource. This study supports a role for rFVIIa as an adjunctive means of achieving hemostasis in patients with life threatening hemorrhage that has failed to respond to surgical measures and blood component therapy. In addition, the use of a simple clinical scoring system may help to predict patient outcome following the use of rFVIIa, and may help reduce the inefficient use of this expensive and effective resource.
This study had a number of strengths and limitations. The accuracy and completeness of the discharge diagnoses and patient medication records in this study can be verified where all data were collected from patient computerized record. The study could provide a nucleus for a Hemostasis Registry to be source of data for the off-license use of rFVIIa in the KSA. Furthermore, given the critical situation of the patient population it would be difficult to conduct a prospective study thus it was done retrospectively.