Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2016) Volume 4, Issue 4
Objective: To validate a smartphone application-based clinical decision support system (CDSS) for risk assessment of venous thromboembolism (VTE) in hospitalized medical patients.
Setting: The medical department of a teaching hospital in Jeddah, Saudi Arabia. Participants: 97 patients, admitted to the medical ward during the month of December 2015.
Aim of the study: A smart phone application based CDSS was developed to assess the risk of VTE in medical patients. Patient data were collected and risk of VTE was calculated simultaneously by the application and by an expert hematologist. The aim of the study was to determine agreement between both sources.
Results: Ninety-seven patients, mean age 50 (19-92) and 51% (50) males were included. Forty-eight percent of patients were stratified as high-risk score based on CDSS compared to forty-seven percent based on expert opinion. There was a strong agreement between the CDSS and the expert hematologist opinion, on the indication and type of prophylaxis suggested for patients with a high-risk score (Chi square 86.7 and 155, p= 0.000, p=0.000, respectively). There was also an agreement with expert hematologist on the need for thromboprophylaxis as well as the type of prophylaxis (Chi square 86.7 and 1.55 respectively).
Conclusion: Smartphone application-based CDSS shows a strong agreement with expert opinion for determination of VTE risk score in medical patients. Thus, the smart-phone based CDSS application has the potential to improve physician compliance with guidelines and reduce inappropriate use of thromboprophylaxis, therefore improving clinical care.
Keywords: Venous thromboembolism; Thromboprophylaxis; Clinical decision support system; Smartphone application
Hospitalization for medical illness accounts for 22% of venous thromboembolism (VTE) cases [1]. The incidence of deep vein thrombosis (DVT) in this population without thromboprophyalxis is 10.5-14.9% [2]. The use of appropriate thromboprophylaxis reduces the risk of DVT by 53%, the risk of pulmonary embolism (PE) by 57%, and fatal PE by 62% [2]. However, the utilization of thromboprophylaxis in a large cohort of 15,000 hospitalized patients was found to be 60% and 40% in another study [3,4]. Moreover, in a tertiary center in a developing country, the percentage of hospitalized medical patients on thromboprophylaxis was much lower at 12.5% [5].
Various interventions were studied to improve adherence to clinical guidelines for thromboprophylaxis in medical patients. A systematic review of available interventions found that education and alerts were effective in improving prescription of appropriate thromboprophylaxis in hospitalized patients [6].
Multifaceted interventions were significantly associated with better outcomes. Clinical Decision Support Systems (CDSS) can serve as handy tools that allow clinicians to access available evidence and help formulate clinical decisions. Adherence of healthcare providers to venous thromboembolism guidelines was previously shown to improve following the introduction of a CDSS to a tertiary Centre. Furthermore, there was a significant reduction of hospital acquired venous thromboembolism (VTE) [7].
This study aims to validate a CDSS developed at King Abdulaziz University hospital, for risk assessment of VTE and recommendation of thromboprophylaxis in patients admitted for medical care.
The study was conducted at King Abdulaziz University Hospital following approval of the hospital ethical committee.
Exclusion criteria
Patients admitted with a diagnosis of acute DVT and/or PE and patients with active cancer were excluded from the study. Ninety-seven consecutive patients admitted to the medical ward during December 2015 were included. We developed a Smartphone application-based clinical decision support system (CDSS), for assessment of the risk of VTE in medical patients. The application utilizes the Padua score for VTE risk stratification to calculate individual patient risk scores. The choice of thromboprophylaxis is determined based on the American College of Chest Physicians (ACCP) guidelines. Heparin contraindications and patients renal functions are taken into consideration.
Medical students trained to use the application by one of the application developers entered individual risk factors for each participant in the CDSS application. Data collected from medical records includes; date of birth, age, recent surgery, immobility, history of active cancer, thrombophilia, cardiac and respiratory failure, acute myocardial infarction, acute infection, rheumatological disorder, hormonal treatment, prescribed pharmacological thromboprophylaxis, heparin contraindications and creatinine clearance (Figures 1-3). Thromboprophylaxis decision created by the CDSS application was compared to the decision of an independent expert hematologist. The expert was blinded to the results of the application.
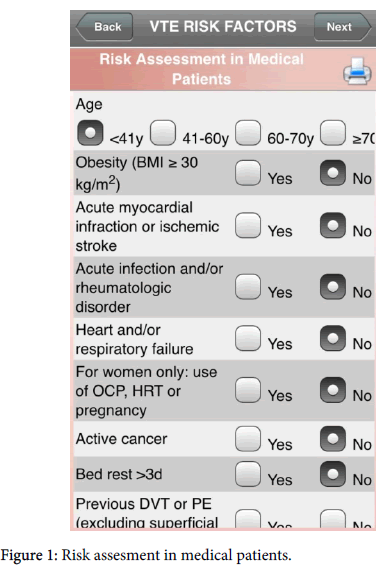
Figure 1: Risk assesment in medical patients.
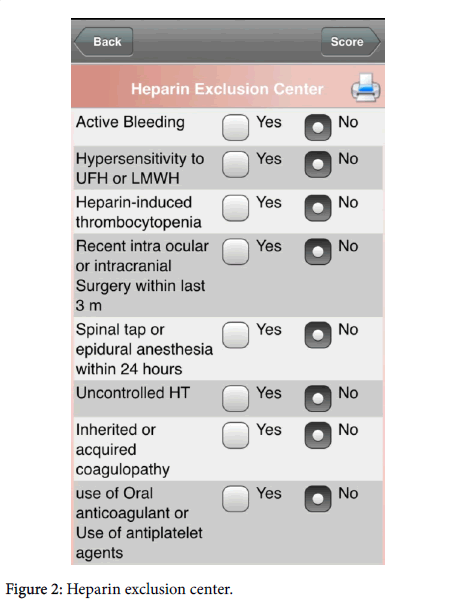
Figure 2: Heparin exclusion center.
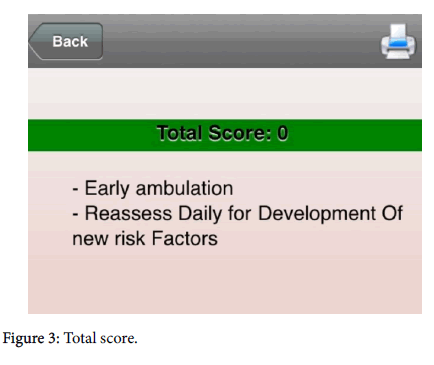
Figure 3: Total score.
Main outcome measure
Agreement on clinical decision determined by the CDSS application, and the expert hematologist.
Statistical analysis
Analysis included all eligible patients. All statistical analyses were performed using SAS version 6.12 computer software (SAS Institute Inc, Cary, NC). When we examined the distribution we found that the data approached to normal distribution (symmetrical), therefore the chi-square test was used to study the agreement between results obtained by the CDSS application and the expert opinion. The percent correlation coefficient was used to study the strength and direction of the relation between both methods used. To calculate the statistical power of the study after it has been conducted, post hoc analysis was performed.
Ninety-seven patients were included in the study. Age ranged between 15 and 92 years (mean age 50 years ± 17.7 years), 51.5% were males (Table 1). Forty-seven percent of patients were stratified as highrisk based on expert opinion and forty-eight percent of patients were stratified as high-risk score based on CDSS. There is a strong agreement between risk stratification based on CDSS and expert opinion (r=0.995=99.5%) (Table 1). Furthermore, thromboprophylaxis decision created by the CDSS application correlated well with to the decision made by an independent expert hematologist for both the indication and type of prophylaxis (Chi square 86.7 and 1.55 respectively) (Tables 2-3). The observed power was found to be 0.989 which means that there is no significant difference between smartphone application and expert opinion regarding the total score, furthermore, by using one-way anova and post hoc analysis the p-value is 0.778 which means no significant difference between smartphone application and expert opinion regarding the indication for treatment.
| Minimum | Maximum | Mean | Std. Deviation | ||
|---|---|---|---|---|---|
| Age | 15 | 92 | 50 | 17.68 | |
| Sex | Frequency | Percent | |||
| Males | 50 | 51.5 | |||
| Females | 47 | 48.5 | |||
| Smartphone | Expert | Pearson Chi-Square | |||
| Number | Percent | Number | Percent | 86.728a | |
| High Score | 47 | 48.40% | 46 | 47.40% | Asymp. Sig. (2-sided) |
| Low Score | 50 | 51.50% | 51 | 52.50% | .000 |
Table 1: Demographic data and number of patients classified as high and low score (high score is=or> 4).
| Expert | Pearson Chi-Square | |||
|---|---|---|---|---|
| Indicated | Not Indicated | 86.728a | ||
| Smartphone | Indicated | 39 | 0 | Asymp. Sig. (2-sided) |
| Not Indicated | 0 | 58 | 0 | |
| Total | 39 | 58 | ||
Table 2: Indication for prophylaxis by Smartphone and expert.
| Expert | Pearson Chi-Square | ||||
|---|---|---|---|---|---|
| Smartphone | UFH | LMWH | None | Total | 155.3 |
| UFH | 25 | 1 | 0 | 26 | Asymp. Sig. (2-sided) |
| LMWH | 0 | 9 | 0 | 9 | 0 |
| None | 6 | 0 | 56 | 62 | |
| Total | 31 | 10 | 56 | 97 | |
Table 3: Type for prophylaxis by Smartphone and expert (UFH: Unfractionated Heparins, LMWH: low molecular weight Heparins).
Venous thromboembolism (VTE) is a significant problem for hospitalized medical patients leading to the possibility of PE and risk of death [8]. The prevalence of autopsy-proven pulmonary embolism in hospitalized medical patients is 2.5% [9]. The risk of thrombosis in a hospital patient depends on individual patient risk factors including acute clinical presentation. Accurate estimation of the risk of thrombosis by health care providers without the aid of risk assessment tools is not easy [10]. The Paudua scoring system helps to classify patients into low or high risk for developing VTE [11]. A number of clear evidence-based guidelines (EBG), are available for thromboprophylaxis in medical patients [12,13].
There is growing awareness of the risk of VTE among hospitalized medical patients and the critically ill, and the use of thromboprophylaxis in this population is increasing [14,15]. Despite the availability of EBG for thromboprophylaxis, evidence suggests that these guidelines are underutilized [16,17]. Causes for under-utilization include variability in clinician knowledge of risk assessment and appropriate prophylaxis and lack of motivation regarding the need for prophylaxis [18]. Ageno et al. documented relatively poor prophylaxis practice for medical patients in 2 Italian hospitals where despite passive dissemination of guidelines only 46% of medical patients received appropriate prophylaxis [18]. A combination of multiple active compliance strategies are likely to be more effective for implementation than a single active strategy [19-21].
Computer-based clinical decision support systems (CDSSs) are defined as any software designed to directly help in clinical decisionmaking [22]. Patients characteristics are matched to a computerized knowledge for the purpose of generating patient-specific real-time recommendations [22]. It can perform complex evaluations and has the advantage of providing active reminders to the clinician and can also help minimize errors made by clinicians. Moreover, it can provide a method of continuing medical education and help improve physician compliance with the guidelines [23]. The first prominent computerbased clinical consultation system was MYCIN, which was designed to function as an aid for infectious disease diagnosis and therapy selection [24]. A critical area relevant to all medical CDSS is validation and evaluation. Accuracy of the clinical decision is the most important element to be evaluated [24]. Therefore CDSSs should be evaluated before widespread use in clinical practice. The Food and Drug Administration (FDA) issued guidance for the validation of medical device software to ensure accuracy, reliability, and consistent intended performance and it should be conducted using an independent expert opinion [25].
The aim of developing this CDSS application is to guide physicians through the systematic assessment of the risk of VTE in individual patients. Consequently, the application will determine the total score and prescribe the appropriate thromboprophylaxis in a few seconds. The CDSS application decision is based on the Padua VTE risk scoring system. Data is fed to the application in the form of yes or no responses, entered by pressing radio buttons in each group of questions. In order for the total score to be calculated, all questions must be answered. Following that, the choice of thromboprophylaxis will be determined based on the answers to a list of yes or no questions including the patient’s most recent creatinine clearance. Thus, the application recommends the type of thromboprophylaxis whether mechanical or pharmacological, based on individual patient data. If pharmacological thromboprophylaxis is recommended, details including class of medication, dose, frequency, mode of administration are provided. Results indicate that the risk score, indication and type of thromboprophylaxis derived from the CDSS application agreed well with the expert hematologist’s opinion. By using Chi square we can't reject the null hypothesis by Alpha=0.05. The correlation between the expert opinion and the application there is a strong positive correlation of 99.5%. Tooher et al. assessed the effectiveness of different strategies for improving the uptake of prophylaxis for VTE in hospitalized patients [19]. A number of active strategies were evaluated including computer-based. While all strategies resulted in improvement of the thromboprophylaxis practice, the most effective strategy for increasing adherence to guidelines appeared to be the CDSS. Implementation of clinical guidelines for venous thromboembolism prophylaxis through a CDSS used in an orthopedic surgery department was found to change physician attitudes and improve compliance with guidelines [26]. Fagot et al. reported that the provision of a patient-specific prescription order improved compliance with guidelines and the accuracy of prescription for VTE prophylaxis [26].
Leonardo’s project utilized a software for data collection and clinical decision making based on implemented guidelines and recommendations aimed to improve patient health outcomes and promote appropriate resource utilization. It provided automatic alerts and reminders regarding the health status of individual patients, and summary reports that could facilitate specialist visits. An initial assessment is conducted by the care manager to gather information from the patient to develop an individualized care plan. The specialist would review the patient’s system-generated decision and validate it. The project tried to highlight the importance of new professional care figures able to fill the great deficiency in the health care system. It demonstrated the feasibility of incorporating care managers into the health care system to support specialists in the management of patients [27].
In general, it would appear that CDSS are among the most effective strategies for improving prescription practices, which may be due to accessibility and the availability of automated reminders. CDSS applications guide clinicians to prescribe the appropriate thromboprophylaxis and minimize errors made by clinicians with variable experience, knowledge, and motivation for VTE prevention.
It can help to fill the great deficiency in specialized health care providers and help to minimize the gap between the release of the guidelines and its proper dissemination and utilization.
This study included 97 patients and was limited to a single center, thus our experience may not be generalized to other centers. However, once the CDSS is available for download, it could serve a larger patient population, in diverse settings throughout the entire health care system. Recommendation for follow up studies: post implementation outcome studies are recommended.
Special thanks for Dr. Grigoris Gerotziafas, Department of Haemostasis, Hôpital Tenon, France for reviewing this article.