Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2014) Volume 3, Issue 3
A total thyroidectomy was performed on a 62 year-old male patient with 3.5 cm cold nodule and diagnosis of
differentiated thyroid carcinoma was made. He received 200 mCi of I-131 because pulmonary metastases were founded on computed tomography and his serum thyroglobulin level was high (>300 ng/ml). Post-therapy planar whole body scan showed diffuse pulmonary tracer accumulation consistent with pulmonary metastases, 3 foci of activities in the thyroid region of neck and physiological tracer uptake in the liver. Initially, it was considered that high serum thyroglobulin level was caused by pulmonary metastases and activities in the neck were due to residual thyroid tissue. But, single photon emission computed tomography/computed tomography (SPECT/CT) images demonstrated that the activity in the midline of the neck was originated in the cervical (C5-6) vertebra due to bone metastasis. Cervical vertebra metastasis in the same level with probable residual thyroid tissue in planar I-131 whole body scan can be easily overlooked. We considered that the complementary SPECT/CT for head and neck region should be used not only in the selected differentiated thyroid patients with unexpected abnormal activity
but also in patients with expected residual thyroid tissue, salivary gland or mouth activity in planar I-131 whole body scan.
Papillary thyroid carcinoma (PTC) is the most common malignancy of thyroid gland and it constitutes up to 85% of all thyroid cancers [1]. In general, prognosis of this tumor is good but certain histologic subtypes such as oncocytic variant have a worse prognosis as compared with classical variant [2]. Initial treatment for thyroid carcinoma is near-total or total thyroidectomy to remove the primary tumor with or without neck dissection [3]. Postoperative management includes high-dose I-131 administration for both treatment and diagnostic purposes. The goal of radioiodine therapy is ablation of normal residual thyroid tissue and destroying distant metastases. Following this therapy, measurement of serum thyroglobulin and planar I-131 whole body scan (WBS) to detect residual thyroid tissue and metastases are routine diagnostic procedures in patients with differentiated thyroid carcinoma (DTC) [4]. However planar I-131 WBS sometimes fails to correctly define the location of I-131 avid foci. One of the major problems is differentiation of physiologic sites from pathological lesions particularly in the neck region. Because normal residual thyroid tissue and salivary glands are main physiologic sites in post-therapy I-131 WBS, an abnormal I-131 avid focus can overlap with normal structures [5,6]. Single photon emission computed tomography/computed tomography (SPECT/CT) combined with planar I-131 WBS provides morphological information and it is significantly more accurate for diagnosis and staging than conventional planar WBS [7].
The patient was 62 year-old man presented with 3.5 cm cold nodule. A total thyroidectomy was performed and PTC (oncocytic variant) was diagnosed histopathologically. After the operation he was hypothyroid with a serum thyroglobulin level of >300 ng/ml and serum thyroid stimulating hormone (TSH) of 82 mIU/L. Ultrasonography was performed and minimal soft tissue was founded in the thyroid region but it couldn’t differentiate residual thyroid tissue from postoperative granulation tissue. In addition, multiple pulmonary nodules were founded on CT. Then he referred to our institution for high dose I-131 treatment. He received 200 mCi of I-131 for ablation of residual thyroid tissue and destruction of distant metastases. Eight days after the treatment of I-131, planar I-131 WBS was performed in anterior and posterior projections using dual-head gamma camera, Infinia Hawkeye (GE Healthcare®). High energy, parallel-hole collimators were used. During the same session, complementary SPECT/CT images over the head and neck region were obtained using Infinia Hawkeye (GE Healthcare®) equipped with integrated x-ray transmission system (low-dose CT) to provide morphologic information.
In the evaluation of planar I-131 WBS, diffuse pulmonary tracer accumulation consistent with pulmonary metastases, 3 foci of activities in the thyroid region of neck and physiological tracer uptake in the liver were founded (Figure 1A). Initially it was thought that high serum thyroglobulin level was only caused by pulmonary metastases and activities in the neck were due to residual thyroid tissue. However, transversal CT (Figure 1B) and fused SPECT/CT (Figure 1C) images demonstrated that the activity in the midline of the neck (Fig. 1A black arrows) was originated in the cervical (C5-6) vertebra due to bone metastasis (Figure 1B-1C white arrows). The other two foci of activities in the neck were consistent with residual thyroid tissue.
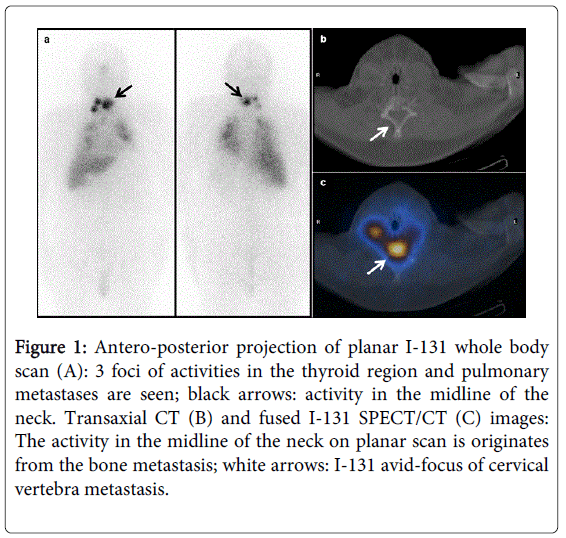
Figure 1: Antero-posterior projection of planar I-131 whole body scan (A): 3 foci of activities in the thyroid region and pulmonary metastases are seen; black arrows: activity in the midline of the neck. Transaxial CT (B) and fused I-131 SPECT/CT (C) images: The activity in the midline of the neck on planar scan is originates from the bone metastasis; white arrows: I-131 avid-focus of cervical vertebra metastasis.
Planar I-131 WBS after I-131 treatment is routinely performed to determine residual thyroid tissue or metastases of DTC. But the accurate localization of abnormal foci of activities is not possible usually because of the lack of anatomic landmarks. In addition, physiological I-131 uptake in the salivary glands, nose, mouth and residual thyroid tissue is also an important problem because some abnormal foci of activities can be hidden by these overlapping structures [8-11]. In some studies, SPECT/CT was performed on only selected patients whose planar images showed inconclusive findings [11,12]. Chen et al. [11] reported that SPECT/CT was of incremental value over planar I-131 WBS in increasing accuracy, reducing pitfalls and modifying therapy in 73.9% of patients with DTC. In this study, uncommon metastatic lesions were found in 9 of 66 patients with regard to SPECT/CT. A case with a posterior skull lesion which was hidden by physiological structures and identified by SPECT/CT was reported by Sioka et al. [6]. Tharp et al. [5] reported that SPECT/CT imaging changed the localization of I-131 avid foci in the neck region in 5 of 14 patients; from thyroid bed to lymph node in 2 patients, from lymph node to thyroid bed in 2 patients and from lymph node to a metastasis in the cervical vertebra in one patient.
In our patient, on the planar I-131 WBS, cervical vertebra metastasis mimicks residual thyroid tissue, so the activities in the thyroid region can easily be reported as residual thyroid tissue if SPECT/CT over the neck region is not applied routinely. For this reason, we consider that the complementary SPECT/CT for head and neck region should be used not only in the selected DTC patients with unexpected abnormal activity but also in patients with expected residual thyroid tissue, salivary gland or mouth activity in planar I-131 WBS.
Complementary SPECT/CT to planar I-131 WBS should be used to improve the planar data interpretation, correctly localizing I-131 avid foci and differentiating between abnormal and physiological structures. This report highlights the value of SPECT/CT which is very efficacious in clarifying confusing abnormalities particularly in the neck region.