Journal of Molecular Imaging & Dynamics
Open Access
ISSN: 2155-9937
ISSN: 2155-9937
Research Article - (2018) Volume 8, Issue 1
Keywords: Endotracheal intubation; Ultrasonography; EmergencyDepartment
Airway management is the most important step in critical illness [1]. The correct placement of the ET provides the absolute continuity of the airway. Especially in emergency medical clinics, incorrect tube placement that can't be identified increases mortality and morbidity. In the studies performed, the defined incidence of esophageal intubation varied between 6-16% [2]. Location of ET; should be verified immediately after intubation with both clinical evaluation and assistive devices. In the literature, in addition to clinical evaluation, the most reliable method for confirming and monitoring the location of the ET is the continuous wave capnography [3]. The use of USG is expanding in emergency departments, intensive care and anesthesia departments due to its advantages such as safe, fast, reproducible, wide use and simultaneous imaging and maximum benefit in airway management [4]. USG, bilateral diaphragm movements, pulmonary atrophy associated with pleural movement of the lung, imaging of the tracheal tube, and ET were used to confirm the location [5]. In our study, we compared USG with auscultation and waveform capnography to confirm ET site in emergency medicine clinic; it is aimed to evaluate the effectiveness of USG in airline safety.
Approval was granted by the Local Ethics Committee before beginning the study. It was designed as a prospective, single-center, clinical observational study. Emergency medical specialists and assistants who USG training were included in the study. These specialists and assistants were trained in lung and trachea sonography. All patients over 18 years of age who were admitted to the emergency service with arrested or intubated for medical reasons (airway safety, low GCS, elevated PCO2, low PO2) were included in the study. Patients under 18 years of age, known pneumothorax and open wound on the spine, patients with impaired neck integrity and tracheostomy were not included in the study. Verification of intubation location; in accordance with current international guidelines, under the supervision of an emergency medical specialist who manages the operation, through clinical evaluation and waveform capnography. In the clinical evaluation, the right and left hemithorax and epigastric region were auscultated. In the auscultation, right and/or left breathing sound was accepted as Endotracheal intubation. Breathing sound from the epigastric region was considered as stomach intubation. USG, after intubation, suprasternal area, S6 model device of Sonoscape brand was performed with 4.5-11 MHz superficial probe. Horizontal plane; single lumen imaging endotracheal intubation, double luminal imaging esophageal intubation. When the patient is ventilated for clinical confirmation of intubation; right and left hemithorax, midclavicular line, on the nipple, and the pleural shear motion with the superficial tissue probe on the vertical plane. Simultaneous right ventricular and/or left pleural gliding movement was interpreted in favor of endotracheal intubation. The absence of simultaneous bilateral pleural shift with ventilation was interpreted in favor of esophageal intubation. Entidal CO2 was measured by means of a wave-form capnograph with Masimo Emma. It was accepted that EI was present if the value after at least five ventilations was greater than 4 mmHg in waveform capnography and if characteristic waveform was present. Statistical analysis of the data obtained in the study was made using SPSS statistical software version 15.0 (SPSS Inc. Chicago, IL, USA). Descriptive statistics were calculated as mean ± standard deviation, median (minimum, maximum, frequency and percentage). The sensitivity, specificity, negative and positive predictive values of the comparative methods (in NPV, PPV, respectively) were calculated. Statistical significance was accepted as p < 0.05 for all analyzes.
112 patients were admitted to the Izmir Bozyaka Training and Research Hospital Emergency Medicine Clinic. Thirty-seven of these patients met the inclusion criteria (Figure 1).
Figure 1: Flow chart of study.
21 patients of them arrest, 2 patients were admitted due to low GCS, 12 patients for airway safety, 1 patient for low PO2 and 1 patient for intubation tube replacement (Table 1). Of the 37 patients included in the study, 18 (48.6%) were female. The mean age of the patients was 71.86 ± 14.74. EtCO2 values were recorded after 37 patients were consented. The mean value of the measured values was 22.35 ± 13.34 mmHg (Table 2).
| Variables | Number (n) | Percent (% ) |
|---|---|---|
| Traumatic arrest | 2 | 5.4 |
| Non-traumatic arrest | 19 | 51.4 |
| Low GKS | 2 | 5.4 |
| Airway safety | 12 | 32.4 |
| Low pO2 | 1 | 2.7 |
| Other | 1 | 2.7 |
| Total | 37 | 100.0 |
Table 1: Reasons for intubation of the patients studied.
| Age mean ± SD. year | 71.86 ± 14.74 |
| Sex, n (%) | |
|---|---|
| Woman | 18 (48.6%) |
| Male | 19 (51.4%) |
| EtCO2. mean ± SD. mmHg | 22.35 ± 13.34 |
Table 2: Demographic and clinical characteristics of the patients studied.
In our study, we observed that augmented auscultation, which is used as a gold standard for waveform capnography and clinical evaluation, shows high correlation. (Pearson Correlation Sign: 0.881, p and lt; 0.05)
During the study, 37 patients were enrolled. 33 intubations were determined to be tracheal in the first attempt. Tracheal USG identified 32 of these intubations as tracheal intubation. The tracheal USG identified 1 of these 33 tracheal intubations as esophageal intubation (False positive). No false negatives were detected (Table 3).
| Variables | Capnograph Esophagus, n (%) | Capnograph Trachea, n (%) | Total, n (%) |
|---|---|---|---|
| USG esophagus, n (%) | 4 (10.8) | 1 (2.7) | 5 (13.5) |
| USG trachea, n (%) | 0 | 32 (86.5) | 32 (86.5) |
| Total, n (%) | 4 (10.8) | 33 (89.2) | 37 (100) |
Table 3: Recognition of esophageal intubation with tracheal USG.
Sensitivity and specificity of tracheal USG; sensitivity was 100% (95% CI, 40.23-100%), specificity was 96.97% (95% CI, 84.18-99.49%), positive predictive value (PPV) was higher than waveform capnography as the gold standard) was found to be 80% (95% CI, 28.81% to 96.70%) and negative predictive value (NPV) to 100% (95% CI, 89.01% to 100%). The kappa value for this evaluation was calculated as 0.87. This indicates a high level of coincidence (Table 4).
| Variables | Tracheal USG |
|---|---|
| Sensitivity (95% CI) | 100% (40.23 - 100%) |
| Specificity (95% CI) | 96.97% (84.18 – 99.49%) |
| PPV (95% CI) | 80% (28.81- 96.70%) |
| NPV (95% CI) | 100% (89.01 - 100%) |
| Kappa | 0.87 |
| CI: Confidence Interval; PPV: Positive Predictive Value; NPV: Negative Predictive Value. | |
Table 4: Sensitivity and specificity of tracheal USG according to capnography with detection of esophageal intubation.
Intubation was evaluated by pleural shear motion with USG. Pleural shear motion, 33 tracheal intubations; 32 as tracheal intubation and 1 as false positive esophageal intubation. 4 esophageal intubations, 3 as esophageal intubation. 1 esophageal intubation as false negative as tracheal intubation (Table 5).
| Variables | Capnograph esophagus, n (%) | Capnograph trachea, n (%) | Total, n (%) |
|---|---|---|---|
| Pleural œsophages, n (%) | 3 (8.10) | 1 (2.7) | 4 (10.8) |
| Pleural trachea, n (%) | 1 (2.7) | 32 (86.5) | 33 (89.2) |
| Total, n (%) | 4 (10.8) | 33 (89.2) | 37 (100) |
Table 5: Recognition of esophageal intubation by pleural slip image.
Sensitivity and specificity of pleural shift movement assessed by USG; when compared to waveform capnography as the gold standard; sensitivity 75% (95% CI, 20.34% to 95.88%), specificity 96.97% (95% CI, 84.18% to 99.49%), positive predictive value (PPV) 75% (95% CI, 20.34% to 95.88%) and the negative predictive value (NPV) was 96.97% (95% CI: 84.18% - 99.49%). In this evaluation, the kappa value was calculated as 0.72 (Table 6).
| Variables | Pleural layer |
|---|---|
| Sensitivity (CI 95%) | 75% (20.34% - 95.88%) |
| Specificity (CI 95%) | 96.97% (84.18% - 99.49%) |
| PPV (CI 95%) | 75% (20.34% - 95.88%) |
| NPV (CI 95%) | 96.97% (84.18% - 99.49%) |
| Kappa | 0.72 |
| CI: Confidence Interval; PPV: Positive Predictive Value; NPV: Negative Predictive Value | |
Table 6: Sensitivity and specificity of pleural deposits according to capnography in determining esophageal intubation.
Observation of auscultation and chest wall movements in confirming tracheal intubation is the most commonly used method, but these methods require chest compressions to be stopped during CPR. Waveform capnography is accepted as the gold standard. But; waveform capnography requires ventilation and pulmonary blood flow. Patients with a full stomach with false positive results due to gastric CO2 production; airway obstruction, pulmonary edema, etc. [6-8].
USG is portable, reproducible, low cost, emergency medicine clinics, intensive care, and even in the field is a method that is widespread, makes use of USG in airline management a remarkable method. In addition, USG images are not affected by low pulmonary flow. The USG can determine that the tube is esophagus, without ventilating the patient, and avoid unwanted effects [2]. If the USG is proven to be as sensitive and specific as the waveform capnograph in ETT site validation, it can be used where there is no capnography.
In our study, tracheal USG incorrectly defined tracheal intubation in a patient as esophageal intubation (false positive). In the work Abbasi and his friends have done; it has been reported that this condition may be due to anatomic factors such as thyroid calcification, and that some of the erroneous findings may be corrected by experience, even if not under the control of the user [9].
Comparing the pleural shear motion seen with USG and waveform capnography in confirming the tube location; sensitivity was 75% (95% CI, 20.34% to 95.88%) and specificity was 96.97% (95% CI, 84.18% to 99.49%). Pleural shear motion with USG was not as effective as tracheal USG in confirming ETT location. This is because; the pleural shear motion may be imitated by the physiological condition called the lung pulse. Pulmonary pulse, heart beat occurs at the end of the pleural effect. It moves vertically in a manner compatible with the pleural heartbeat. The lung pulse can be used to identify atelectasis or to exclude the pneumothorax. The lung pulse is more prominent when there is no pleural shift. When there is no pleural shift movement, the pulmonary pulse may mimic pleural shift. USG users should pay attention to this situation [10].
In this prospective study in emergency medicine clinic, waveguide capnograph was encountered in the USG with the USG in confirming the location of the ETT and in the auscultation methods and in the existing guidelines for advanced life support. In our study, the sensitivity of tracheal USG to detecting esophageal intubation was found to be 100% (95% CI, 40.23% - 100%) and 96.97% (95% CI, 84.18% - 99.49%) of specificity. The auscultation, which is the clinical method that we used to determine the location of the tube, was highly correlated with the waveform capnography. In these findings, tracheal USG may be an effective method of confirming ETT location. Like our study, we compared the rapid tracheal ultrasound exam (T.R.U.E.) and quantitative waveform capnography in a prospective observational study by Chou et al. USG has been shown to have high sensitivity and specificity in tube site fixation. In the same study, Chou and colleagues found that real-time USG performed during CPR was an adequate method of confirming the tube location and resulted in a break in the chest press [2].
Because of our current studies and our work, it can be said that the use of USG in the tube location verification at EI is reliable. However, there is a need for further work in this regard (Figures 2-6).
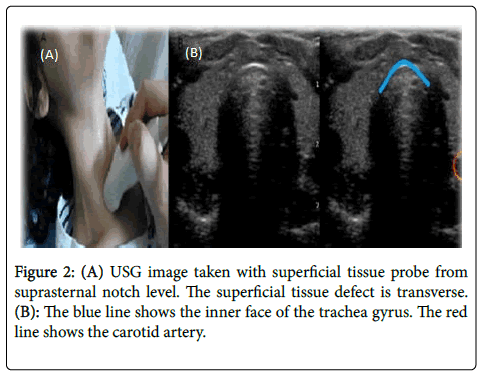
Figure 2: (A) USG image taken with superficial tissue probe from suprasternal notch level. The superficial tissue defect is transverse. (B): The blue line shows the inner face of the trachea gyrus. The red line shows the carotid artery.
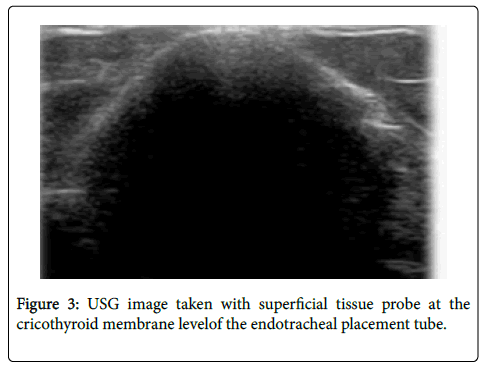
Figure 3: USG image taken with superficial tissue probe at the cricothyroid membrane levelof the endotracheal placement tube.
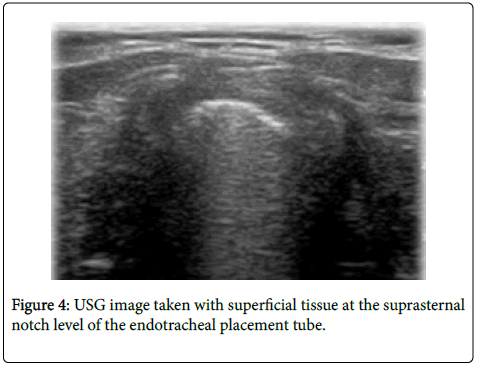
Figure 4: USG image taken with superficial tissue at the suprasternal notch level of the endotracheal placement tube.
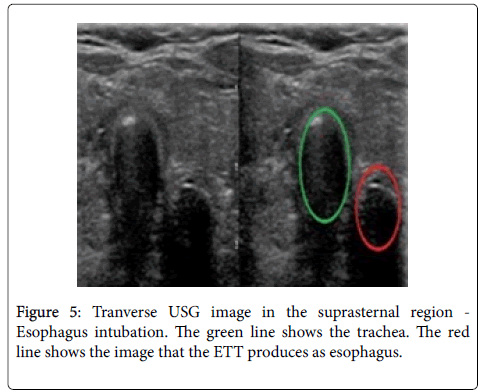
Figure 5: Tranverse USG image in the suprasternal region - Esophagus intubation. The green line shows the trachea. The red line shows the image that the ETT produces as esophagus.
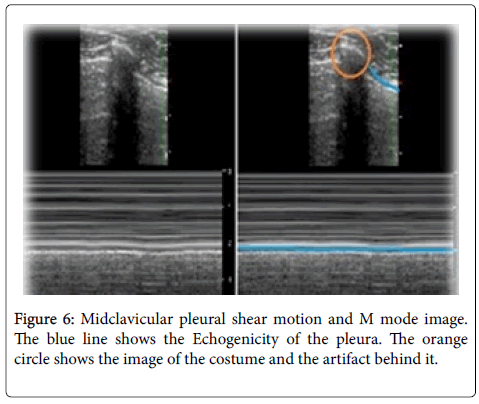
Figure 6: Midclavicular pleural shear motion and M mode image. The blue line shows the Echogenicity of the pleura. The orange circle shows the image of the costume and the artifact behind it.
Our work has some limitations. Our study was carried out in a single-center emergency medical clinic. For this reason, the number of patients and the number of esophageal intubations is low. USG has not been able to assess the reliability of out-of-hospital areas from potential use areas for airway management purposes.
We also could not get enough information about the reliability of the USG in confirming the tube location in this age group because we do not take our patients under 18 years of age. Patients physical characteristics such as weight, body mass index, subcutaneous fat tissue may affect the accuracy of USG. However, we did not evaluate these criteria in our study. Variations in neck anatomy also affect imaging quality and accuracy. While USG users have basic training, USG is user-dependent. For this reason, the difference in interpersonal skills affects the results.
We concluded that USG made with suprasternal notch level line probe had high sensitivity and specificity in determining esophageal intubation. Verification of USG as a supportive method in confirming the location of endotracheal intubation can help early detection of esophageal intubation and prevention of complications. However, more work needs to be done on the USG's tube location verification.
The author declares that there was no financial payments or other benefits from any commercial entity. There is no funding resource supporting the work submitted.