Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Short Article - (2013) Volume 2, Issue 4
Sleep-related violence has been described as “aggressive behaviour arising out of disturbance or dysfunction during the sleep state that results in the physical harm of people or destruction of objects in the physical environment” [1]. A variety of medical, psychiatric and primary sleep disorders can manifest with potentially dangerous behaviour during the night. If not recognized and treated, serious harm or even death can result.
There are three main states of being: wake, Non-Rapid Eye Movement (NREM) sleep and Rapid Eye Movement (REM) sleep. Nocturnal violence can arise during any of these states. At times it can be difficult to determine whether an individual is awake and acting consciously, awake with some degree of cognitive impairment, or asleep with involuntary or unintended actions at the time of a violent act. Violence during sleep is, therefore, differentiated by the state of being during such actions and determined by whether the act was conscious or unconscious. Abnormal activities occurring during sleep, or parasomnias, are disruptive sleep disorders secondary to arousals or partial arousals from sleep or transitions among the different sleep stages. Sleep related violence is a unique, likely under-recognized parasomnia, which can manifest from aggressive gestures to significantly dangerous behaviours. The aim of this review is to provide an overview of violence during sleep and provide diagnostic and treatment strategies for these disorders.
Although difficult to accurately assess due to under-reporting, violent acts are present in up to 3-5% of the general population. Of the epidemiologic studies that have assessed sleep-related violence, the one factor that seems to be consistent is that male gender is associated with an increased prevalence [2-4]. It is not well understood whether this is because sleep related violence truly occurs more often in men or if it is because men tend to experience more violent dreams and the resultant harm may be more significant. In the military population that we treat, sleep-related violence is almost exclusively a male phenomenon even though women are increasingly exposed to combat situations.
Ohayon et al. [5] conducted the two largest studies describing violence during sleep. In 1997, the authors reported that 2% of the 2078 men and 2894 women surveyed from a general population reported they had engaged in a violent act at least once when asleep [5]. Those who reported violent behaviours were also more likely to experience night terrors, daytime somnolence, somniloquy (sleeptalking), bruxism, hypnagogic hallucinations and hypnic jerks. Lifestyle factors associated with these events included an increased likelihood of smoking, caffeine use, and drinking alcohol close to bedtime. In 2010 the authors increased their sample size and conducted 19,961 telephone questionnaires in a general population. They discovered the reported prevalence of sleep related violence was 1.6%. Violent behaviours while asleep were more common in young adults less than 35 years of age. The majority (78.7%) of those with reported violent behaviours while asleep also reported vivid dream recall and 72.8% had other symptoms of parasomnias. Somnambulism (sleepwalking) and sleep terrors were commonly associated and had odds ratios of 2.0 and 4.2, respectively. Approximately 1/3 of those endorsing violent behaviours reported significant harm to themselves or others as a result of the act. A family history of violent behaviour during sleep was highly correlated with an odds ratio of 9.3 [6]. Only 12.3% consulted a physician for these behaviours.
NREM sleep is divided into stage 1 sleep (N1), stage 2 sleeps (N2), and slow wave sleep (SWS, N3). During stage 1 sleep, a patient can be easily awakened although they may seem confused or tired for a few seconds. Stage 2 sleep comprises a majority of the night and is associated with a higher arousal threshold than stage 1 sleep. Attempting to wake a patient from stage 2 sleep is more difficult and the post-arousal amnestic period is longer. SWS is a state of deep sleep and is the most difficult stage to arouse from. A partial awakening during SWS can results in a confusional arousal leading to unintentional or unconscious behaviour and activities, such as somniloqy (sleep talking), somnambulism (sleep talking), or night terrors.
Disorders of arousal have been described as an oscillation or dissociation between the wake and NREM state [7-9]. Other authors have used the terms “partial arousal” and “stuck between sleep and wakefulness”. The American Academy of Sleep Medicine has defined these as “incomplete awakenings” from NREM sleep characterized by reduced vigilance, impaired cognition, retrograde amnesia for the event, and variable motor activity, ranging from repetitive and purposeless movements to more complex behaviours such as eating, drinking, driving, sexual intercourse and aggression [10]. They most commonly arise from SWS and, as such, typically occur during the first half of the night when the proportion of SWS is the highest. Confusional arousals are quite common in children, but may persist into adulthood. It is uncommon for SWS parasomnias to emerge during adulthood de novo, and precipitating factors, such as recreational drugs and alcohol, or alternative medical and psychiatric diagnoses should be considered in these cases [11,12]. Parasomnia events are often associated with predisposing and precipitating factors. Recent stress, sleep deprivation, alcohol use or erratic sleep-wake schedules may play a role in precipitating or exacerbating an event. Other sleep disorders that increase sleep fragmentation, such as Obstructive Sleep Apnea (OSA) or Restless Legs Syndrome (RLS) can also precipitate a confusional arousal.
NREM parasomnias with the potential for violence can be classified as either primary disorders of the sleep states or sleep state transitions, or secondary to pathologic conditions or external influences that emerge during sleep and/or disrupt normal sleep. Secondary parasomnias are typically a form of nocturnal frontal lobe epilepsy (NFLE) and are classified as “Parasomnias Due to Medical Condition” by the International Classification of Sleep Disorders [10]. Psychogenic dissociative states that occur during sleep may also result in parasomnia events [13].
For patients with a primary NREM parasomnia, violence tends to be uncommon unless the subject is provoked or suddenly awakened. A review of medical and legal case records from 1859 until 2007 concluded that reported violent behaviours were associated with provocations and/or close proximity in 100% of confusional arousal patients, 81% of sleep terror patients and 40-90% of sleepwalking patients [14].
In secondary NREM parasomnia events, violence may be an unintended consequence of the stereotyped behaviour common to NFLE or the result of activation of primitive defensive behaviours [15]. There are three subtypes of NFLE, nocturnal paroxysmal dystonia, paroxysmal arousals, and episodic nocturnal wanderings. Nocturnal paroxysmal dystonia can present with simple posturing but may also include more complex behaviours such as kicking or rhythmic core body motions. Paroxysmal arousals, on the other hand, tend to be less purposeful and can mimic night terrors. Episodic nocturnal wandering may include features of posturing, complex motor movement and can culminate with somnambulism [16]. NFLE is often successfully treated with anti-epileptic medication such as carbamazepine. However, despite adequate treatment up to 20 % of patients will have refractory seizures. Surgery may offer improved control of seizures in these individuals [17].
Given the potential complexity of the motor activity with some parasomnias events and the difficulty distinguishing these events from a wakeful state, disorders of arousal have been used as legal defense for violence occurring at night. During NREM sleep, there is a deactivation of the normal cortical regions responsible for monitoring and remembering behaviour despite preservation of motor activity. As stated, these patients lack the normal capacity to respond appropriately to the environment and their surroundings. This ability is the most useful means to differentiate parasomnias from a state of wakefulness [18]. Patients with NREM parasomnias may appear awake and can engage in complicated behaviours such as walking or even driving. However, they should not have appropriate interactions with their environment. Despite appearing awake, they are actually quite difficult to arouse and typically appear confused or even violent when awakened. They do not usually recall dreaming prior to their awakening.
Normal REM sleep produces skeletal muscle atonia. Rapid Eye Movement Behaviour Disorder (RBD) is a parasomnia characterized by the loss of normally occurring atonia during REM sleep accompanied by dream enacting behaviour [19]. The diagnosis of RBD requires both REM sleep without atonia (RSWA) during polysomnography as well as a clinical history consistent with dream enactment behaviour. Both criteria are required as RSWA in and of it may not produce complex behaviours, and dream enactment behaviour is present in a variety of disorders to include OSA, NREM parasomnias, Post-Traumatic Stress Disorder (PTSD) or as a consequence of alcohol use. Severe sleep deprivation may also precipitate dream enactment behaviour.
The lack of skeletal muscle atonia allows patients with RBD to act out their dreams without the normal inhibitory and defensive mechanisms present during the conscious state of wake. As such, both violent dreams, and those involving recreational activities and sports, can result in injury to self and others. The most common potentially lethal REM-related behavioural themes are choking or repeated striking of the bed partner. RBD may also co-exist with NREM parasomnias. This “overlap” syndrome can be complex and may result in severe injury [20]. RBD has been used successfully in numerous legal defenses and can be considered a “parasomnia with continuing danger” therefore classifying it a “non-insane automatism” [21].
Idiopathic RBD occurs in the absence of any identifiable underlying neurologic disease. Secondary, or symptomatic RBD results from, or occurs as part of an underlying neurodegenerative disorder. RBD can be precipitated by stroke and can be seen in narcolepsy patients. RBD is also reported as a side effect of SSRIs, mirtazapine, selegiline and cholinergic therapy in patients with pre-existing neurodegenerative conditions [4].
Among older adults, RBD has an estimated prevalence of 0.4- 0.5%. However, the incidence is significantly greater in patients with neurodegenerative diseases such as Lewy body dementia, multiple system atrophy and Parkinson’s disease [22]. Progressive supranuclear palsy has also been infrequently associated with REM behaviour disorder [23]. Multiple sclerosis is not commonly associated with RBD but can be seen when there are brainstem plaques. Over half of all RBD patients are eventually diagnosed with a neurological disease. A review of nearly 600 RBD cases since its formal classification in 1986 revealed a significant male predominance (80.8%) with a mean age of 65.6 years [4]. Other sources cite a slightly younger population (median onset 50- 65 years) [24]. In comparison, NREM parasomnias are more common in younger men. The frequency of RBD episodes is highly variable, ranging from few lifetime occurrences to multiple events nearly every night [25].
In contrast to NREM parasomnias, RBD patients are usually easily awakened and can often recall dream content similar to the observed behaviour. Not all dreams occur during REM sleep, however. Dreaming can occur in all stages of sleep and dream enactment can be seen during somnambulism and sleep terrors. Oudiette et al. studied 43 patients with sleepwalking and observed that short, unpleasant dream-like mentations occurred in 71% of patients [11].
While not exclusive, the events typically occur in the latter part of the night when more REM sleep naturally predominates. Motor activity is usually less complex and shorter in duration than that seen with SWS parasomnias. Prolonged somnambulism is uncommon. RBD patients typically have their eyes closed during their episodes [26].
Recurrent disturbing dreams are a common feature in PTSD. Sleep related violence is more common in patients with PTSD and its association is likely multifactorial. PTSD is associated with sleep fragmentation, and the psychoactive agents commonly used to treat PTSD cause disruption to normal sleep continuity and architecture. Some agents have, themselves, been shown to precipitate RBD events [4].
Violence during sleep often occurs following a particularly distressing dream or nightmare which can evoke a confusional arousal from NREM sleep or dream enacting behaviour during REM sleep. It is often difficult to determine if the physical behaviour manifests during sleep or if a patient wakes up and is confused by his/her surroundings, striking out at the nearest object. Given that a number of PTSD-related nightmares can arise from stage 2 NREM sleep [27,28] it may be more likely for disordered dreaming to result in a confusional arousal in this population. Confusional arousals, though typically seen during SWS, can also be seen during N2 sleep and may be present late into the sleep period [29]. Awakenings from N2 sleep are more abrupt than those occurring in SWS. And, unlike SWS which predominates in the early part of the night, N2 sleep occurs throughout the sleep period. As such, these events share many similar features with, and may be mistaken for RBD.
Common SWS parasomnias, such as somnambulism, may manifest differently in patients with PTSD. There is a paucity of data on the topic, but one study by Hartman et al. examined 22 patients with polysomnographically confirmed sleepwalking. Fourteen patients had no significant psychological trauma, while six had preceding traumatic events and symptoms consistent with PTSD. These patients differed from those without antecedent trauma in that they more commonly reported vivid, dreamlike mental content accompanying the parasomnia behaviour (83% vs. 25%). Those with a history of trauma also reported that the somnambulism was an attempt to flee from an attacker [30]. The inherently vulnerable state of sleep heightens primitive defensive mechanisms. It stands to reason, therefore, that the potential for violence is much greater if the patient feels as if he/she is being threated or has a pre-existing condition that makes them feel more vulnerable.
Other conditions have the potential for sleep-related violence. Obstructive Sleep Apnea (OSA)-pseudo RBD is associated with violent dream enactment and may produce injury to the patient or bed partner. In a case report of OSA-pseudo RBD in which parasomnia behaviours manifested during abrupt respiratory-related arousals from REM and NREM sleep, CPAP was shown to significantly improve these symptoms [31]. Malingering, Munchausen Syndrome, and Munchausen Syndrome by proxy must also be considered in the differential diagnosis of violent sleep behaviours. Figure 1, reproduced from a recent review article by Siclari et al., lists the spectrum of medical and psychiatric disorders associated with sleep related violence [15]. If all other disease entities are ruled out, it is appropriate to consult with legal and forensic experts to determine the appropriate disposition [13].
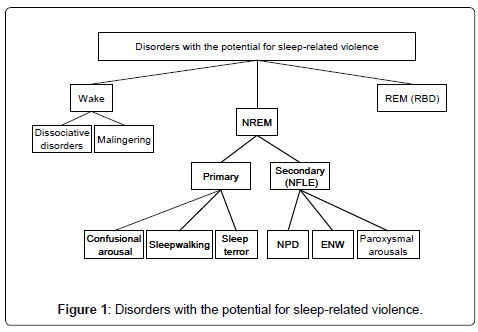
Figure 1: Disorders with the potential for sleep-related violence.
The evaluation of nocturnal violence should begin with a thorough history. When evaluating patients with parasomnias, the first branch point is to distinguish NREM disorders from RBD. Table 1 summarizes the key clinical differences. Most parasomnias are non-violent, so if the only parasomnia behaviour reported is violent or the reason for the encounter is part of a forensic evaluation, the clinician should remain skeptical. Collateral information from the bed partner and other witnesses should always be obtained. Clinical tools such as the Nocturnal Frontal Lobe Epilepsy and Parasomnia Scale and the REM sleep behaviour disorder screening questionnaire can also be helpful [32,33]. Unexplained head trauma in an elderly individual should prompt questioning for RBD. Evaluation of underlying neurological conditions is also important. A detailed neurological exam with appropriate laboratory and radiographic studies may uncover subtle signs of a potentially treatable condition. Neuropsychological testing should be considered when any focal abnormality is discovered or if there are deficits on a mental status examination.
| NREM | RBD | |
|---|---|---|
| Time | Early | Late |
| Memory of event | No | Yes |
| Arousability | Difficult | Easy |
| Post-event confusion | Yes | No |
| Age | Children/Young adults | Elderly |
| Genetic predisposition | Likely | Unlikely |
| Co-morbidities | Usually none | Neurodegenerative disorders |
| Treatment | BZD | BZD |
| Behaviours | More complicated, eyes open | Simple, eyes closed |
Table 1: Features of NREM vs. REM parasomnias.
Polysomnography is an essential component in the evaluation of a patient with suspected violent behaviour during sleep. It can assess motor activity during different stages of sleep and help identify potential causes, such as OSA or nocturnal seizures. A polysomnographic evaluation must include multiple EEG channels to assess for seizure activity as well as video monitoring, and may be required over multiple nights. For RBD, RSWA should be a persistent abnormality. The sleep technologist should be instructed to take detailed notes regarding the patient’s behaviour, especially if the patient moves out of the line of sight of the camera. As previously mentioned, laboratory staff should avoid touching the patient if possible since provocation may precipitate an attack. If the patient awakens, the technologist should ask the patient about any dreams that they can recall. This is helpful in correlating behaviour with dream-enactment. Though patients with NREM parasomnias have mostly normal sleep architecture, polysomnography (PSG) may also uncover a precipitating sleep disorder such as OSA. If there is a low concern for other sleep disorders, the PSG may be performed in the sleep-deprived state in order to uncover parasomnias [34]. If NFLE is suspected, additional daytime EEG may be considered after additional sleep deprivation. If in-lab PSG fails to capture any abnormal behaviour, a longer duration of nocturnal videography may be obtained using home videos [35].
Non-pharmacologic therapies
Behavioural and environmental modifications are the mainstay of treatment for individuals with sleep-related violence. Due to the increased propensity for violent outbursts after sleep deprivation, it is essential to instruct patients on sleep hygiene and ensure that they adhere to a healthy sleep-wake routine. Avoidance of alcohol and other substances is also important in order to minimize violence while asleep. The bedroom should be made as a safe as possible. Particularly, for the NREM parasomnias, it may be necessary to put multiple locks on the bedroom and exterior doors of the house. Door alarms can be effective in alerting family members of a wandering individual. Potentially harmful objects or items that could be used as weapons should be removed. Padding the furniture, especially sharp corners, can also be helpful. Sleeping on the first floor may be required if there is the potential for defenestration. If a family member or caregiver encounters a wandering individual they should be cautious about approaching them due to the risk of a violent outburst upon awakening.
Benzodiazepines
The most heavily prescribed medications for both NREM and REM parasomnias are benzodiazepines, particularly clonazepam. Although one recent retrospective chart review did showed a treatment response rate of 73.7%, [36] most of the data comes from clinical experience and there are few controlled trials to demonstrate the magnitude of the treatment effect.
N Serotonergic medications
It is postulated that serotonin is responsible for the increased muscle tone and inhibition of REM atonia due to actions at the pons or spinal cord. Serotonin reuptake inhibitors such as fluoxetine are associated with increased muscle tone during REM and theoretically may worsen RBD [37]. In contrast, sertraline and paroxetine have been effective treatments for disorders of arousal from NREM sleep [36,38].
Alpha-2-adrenoreceptor modulators
Alpha-2-adrenoreceptors are thought to mediate REM behaviour disorders. A case report by Onofrj et al. postulated that the alpha-2 antagonism of mirtazapine is implicated in REM behavioural disturbance [39]. Another group found that clonidine, an alpha-2 agonist, decreased the frequency of nocturnal outbursts in a case of treatment-refractory sleep-related violence [40].
High dose melatonin
Given that benzodiazepines can worsen sleep disorders such as OSA and can be dangerous in elderly patients at risk for falls, melatonin has been studied as an alternative and has been shown to be effective in retrospective studies [41-43] as well as in a small prospective cross-over study [44]. In many of these studies, doses from 3-12 mg per night were used. A recent survey compared the effectiveness of melatonin (mean dose 6mg per night) with clonazepam (mean dose 0.5 mg per night). Both medications were found to reduce injuries, with the melatonin group showing a more significant reduction. Melatonin also showed an improved safety profile compared with clonazepam. However, the majority of patients continued to have RBD symptoms and only 3 patients in each group reported complete resolution of nocturnal behaviours. (12% in the melatonin group vs. 16% in the clonazepam group). There were no differences in treatment retention, with 28% of melatonin patients and 22% of clonazepam patients discontinuing treatment [45].
Pramipexole
A few studies have shown that dopamine agonism may play a role in ameliorating RBD symptoms. Although the amount of RSWA did not change in these studies, patients did report symptomatic improvement [46,47]. In one study of 15 RBD patients, 80% reported improvement after 1 month of pramipexole therapy. Of the patients that reported improvement, most also reported a reduction or disappearance in nightmares. The authors hypothesized that reduction in REM density or alterations in dream content may have been partially responsible for the decrease in RBD severity [48]. Dopamine is highly linked to dreaming. High doses of dopaminergic drugs are known to induce vivid dreams or nightmares [49,50]. However, low doses of dopamine agonists such as pramipexole may actually reduce nightmares in patients with RBD. Clearly, more research is needed to identify optimal treatment strategies.
Violent behaviour resulting from primary sleep disorders is uncommon but potentially lethal. Recognizing the clinical differences between NREM parasomnias and RBD is important as it can impact both prognosis and treatment plans. Middle-aged or elderly patients with a suggestive history should have a comprehensive evaluation to include a neurologic exam and polysomnography to rule out RBD and potentially early signs of neurodegenerative disorders. Prompt identification of the etiology of the parasomnia, as well as initiation of safety precautions, can limit the morbidity associated with these disorders.
Evaluating patients for sleep related violence in response to criminal charges should not be immediately dismissed as an alibi. It is possible for the first reported event to result in significant injury or assault. However, these events are rarely isolated occurrences and the lack of a prior history of related events or identifiable precipitating factors should raise skepticism.