Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2014) Volume 3, Issue 3
Water clear cell parathyroid adenoma is a rare cause of primary hyperparathyroidism. In this rare disease entity, normal parathyroid tissue is replaced with growth of water-clear cells, instead of the chief cell hyperplasia associated with the majority of parathyroid adenomas. We present the case of a water clear cell parathyroid adenoma in a 54 year old woman with symptomatic hypercalcemia, as well as a review of the literature on this rare disease. This constitutes the 17th reported case of water clear cell parathyroid adenoma.
<Primary hyperparathyroidism is the most common cause of hypercalcemia in the ambulatory setting [1]. In 85% of cases, primary hyperparathyroidism is due to a solitary parathyroid adenoma [1]. Other causes include diffuse parathyroid hyperplasia, multiple parathyroid adenomas and, rarely, parathyroid carcinoma.
Histologically, there are several types of parathyroid adenoma, with chief cell type being the most common. Adenomas can also be composed of oxyphil cell types, lipoadenoma or mixed cell type [2]. The rarest parathyroid adenoma is the water-clear cell type, with only 16 cases reported in the literature.
We present a case of primary hyperparathyroidism due to a solitary water-clear cell parathyroid adenoma in a 54 year old woman.
A 54 year old woman presented with bone pain, fatigue, depression, weakness, and forgetfulness. Serological tests demonstrated hypercalcemia (serum calcium of 12.4 mg/dL), and an elevated serum parathyroid hormone level (PTH) of 130 ng/L indicative of hyperparathyroidism. She had no history of kidney stones and no family history of endocrine neoplasia. Her head and neck examination was within normal limits with no palpable neck mass detected.
Preoperative neck ultrasonography revealed a normal-appearing thyroid gland and a 2.8x1.1x1.1 cm hypoechoic mass located inferior and posterior to the left thyroid lobe consistent with a parathyroid adenoma (Figure 1).
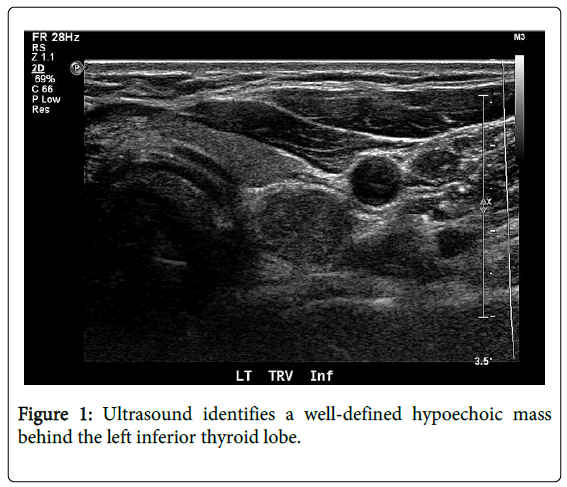
Figure 1: Ultrasound identifies a well-defined hypoechoic mass behind the left inferior thyroid lobe.
A sestamibi scan was also consistent with a left inferior parathyroid adenoma (Figure 2). She underwent a minimally invasive radio-guided parathyroidectomy, during which a tan 2.8 cm mass was found infero-posterior to the left thyroid lobe. The recurrent laryngeal nerve was identified coursing directly over the mass, which was bluntly dissected away from the intact nerve and removed without difficulty. Intraoperative technetium count on the mass was 1200 against a background of 1400, and 20 minutes after removal of the mass, serum PTH had dropped from a peroperative level of 149 ng/L to 29 ng/L. The patient had an uneventful post-operative course.
Pathologic examination of the mass demonstrated a parathyroid adenoma with diffusely clear cytoplasm consistent with a water clear parathyroid adenoma (Figure 3).
Water clear cell parathyroid adenoma is a rare cause of primary hyperparathyroidism; only 16 cases have been reported in the literature. These adenomas are characterized on histology by large clear cells, thought to be transformed from parathyroid chief cells [3]. On microscopic examination, water clear cells have foamy cytoplasm containing vacuoles [4]. These vacuoles are typically 0.2-2 microns in diameter, and although their origin is not entirely known, they are theorized to originate from the Golgi apparatus, endoplasmic reticulum, or mitochondria [5,6]. The transformation from normal parathyroid chief cell to vacuolated water clear-cell is speculated to occur more frequently with advanced patient age [7,8].
Water clear cell parathyroid adenoma must be distinguished from water clear cell parathyroid hyperplasia, in which all four parathyroid glands have water clear cells as their dominant histology. In cases when all four parathyroid glands are examined microscopically, the diagnosis of water clear cell parathyroid adenoma can be readily made if other parathyroid glands are histologically normal. For cases in which only one parathyroid gland is examined, as in the case presented, the diagnosis of adenoma is made when a cuff of normal parathyroid tissue is observed around the water clear cells. Adenoma is confirmed in other cases by resolution of hyperparathyroidism following removal [9].
Among the 17 reported patients with water clear cell parathyroid adenoma, the average age at diagnosis was 57 years (range 18-81). Seven patients were male and ten female. In the 12 patients for which ultrasound were used in the imaging workup, the water clear cell parathyroid adenoma was identified in nine (75%) cases (Table 1).
| Author, Year | Age/Gender | Calcium | PTH | Symptoms | Ultrasound | Nuclear Med | Adenoma |
|---|---|---|---|---|---|---|---|
| Kovacs et al. | 48yo M | 11.8 mg/dL | 4.5 mIU/mL | nephrolithiasis | ND | ND | ND |
| Grenko et al. [18] | 40yo M | 11.3 mg/dL | 945 pg/mL | fatigue, leg cramps | ND | ND | 5.0 cm R superior |
| Begueret et al. [19] | 73yo M | 13.8 mg/dL | 207 pg/mL | nephrolithiasis | ND | ND | 2.8 cm L inferior |
| Dundar et al. [10] | 43yo F | 13.3 mg/dL | 1667 pg/mL | fractures, cramps, fatigue, lethargy | 6 cm L intrathyroidal | Not seen | 6 cm intrathyroidal L lobe |
| Kuhel et al. [5] | 56yo F | 3.3 mmol/L | 52 ng/L | asymptomatic | 2.3 cm R thyroid | Not seen | 2.8 cm R superior, 1.5 cm L superior |
| Kanda et al. [9] | 52yo F | 11.7 mg/dL | 672 pg/mL | nephrolithiasis | 2.6 cm L inferior | L inferior | 6.8 cm L inferior |
| Prasad et al. [20] | 40yo F | 12.4 mg/dL | 346 pg/mL | fatigue, cramps, weakness | ND | ND | 3.0 cm L superior |
| Kodoma et al. [16] | 18yo F | 11.6 mg/dL | 356 pg/mL | nephrolithiasis | 4.5 cm R | Right | 5.0 cm R superior |
| Liang et al. [17] | 59yo F | 11.8 mg/dL | 265 pg/mL | mood changes, lethargy |
Not seen | L superior, R superior | 4.5 cm R superior |
| Papanicolau-Sengos et al. [11] | 64yo M | normal | ND | asymptomatic | ND | ND | 4.7 cm L inferior |
| Bai et al. [6] | 81yo M | ND | 22.2 pmol/L | ND | Not seen | Lower neck | 4.0 cm R superior |
| Bai et al. [6] | 55yo M | ND | 15.9 pmol/L | ND | Not seen | Not seen | 1.4 cm L superior |
| Piggott et al. [14] | 74yo F | 3.13 mmol/L | 488.9 ng/L | abd pain, constipation,lethargy |
4.8 cm L inferior | L inferior | 5.5 cm L inferior |
| Ezzat et al. [15] | 73yo M | 3.24 mmol/L | 30.8 pmol/L | ND | L inferior | L inferior | 3.7 cm L inferior |
| Ezzat et al. [15] | 74yo F | 2.9 mmol/L | 11.8 pmol/L | ND | 1.6 cm L inferior | Not seen | ND |
| Murakami et al. [4] | 59yo F | 11.9 mg/dL | 72.3 pg/dL | nephrolithiasis, gastric ulcer | 0.8 cm L | Not seen | 0.8 cm L inferior |
| Present Case | 54yo F | 12.4 mg/dL | 130 ng/L | bone pain, fatigue, depression, weakness, forgetfulness | 2.8 cm L inferior | L inferior | 2.8 cm L inferior |
Table 1: Seventeen reported cases of water clear cell parathyroid adenoma.
In the 12 patients for which nuclear imaging were used, the adenoma was visible in seven (58%) cases. The average maximum diameter of the adenomas reported to date was 3.8 cm (range 0.8-6.8 cm).
The location of water clear cell parathyroid adenoma has varied in previous reports. One adenoma was intrathyroidal [10] and there has been one report of dual water clear cell parathyroid adenoma [5]. All other cases, however, have reported adenomas in expected anatomic parathyroid locations. To date, water clear well parathyroid adenomas have been reported in one patient with multiple endocrine neoplasia type 1 (MEN-1) and one patient with neurofibromatosis type 1 (NF-1), but all others were sporadic.
Of note, most reported water clear cell parathyroid adenomas are relatively large in size. Kanda et al. [9] hypothesized that water clear cells have low endocrinologic activity, and that calcium levels do not considerably increase until the adenoma is large. Our case of a 2.8 cm adenoma is consistent with previous reports.
The differential diagnosis for water clear cell parathyroid adenoma includes metastatic renal cell carcinoma (RCC), clear cell type [6]. The two entities appear histologically similar, and water clear cells have been reported to stain positively with an RCC monoclonal antibody [6,11]. Further confusing the clinical picture is the fact that RCC can synthesize PTH-related protein and produce the hypercalcemia more commonly seen with parathyroid adenoma [12,13]. These findings stress the importance of a thorough history and physical examination in the workup of any case of primary hyperparathyroidism.
The clinical presentation of patients with water clear cell adenoma is indistinguishable from that of the more common parathyroid adenoma, and the diagnosis is made only on pathologic examination. To date, there have been no reports following complete excision. With more cases of water clear cell parathyroid adenoma identified and reported, this rare cause of hyperparathyroidism can be more completely characterized.
In summary, we report the case of a 54 year old female patient with primary hyperparathyroidism caused by a water clear cell parathyroid adenoma. Water clear cell adenomas are a rare cause of hyperparathyroidism, which can be considered cured after their complete surgical removal.