Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
![]() +44 1478 350008
+44 1478 350008
ISSN: 2167-0277
![]() +44 1478 350008
+44 1478 350008
Review Article - (2013) Volume 2, Issue 6
Willis-Ekbom disease (WED), also known as restless legs syndrome, is generally accepted as a disease of unknown pathophysiology, though it is believed that dysfunctions in the dopaminergic system and iron metabolism may play a role. However, an increasing body of evidence points to the insufficient modulation of thyrotropin hormone by the neurohormone dopamine (DA) as the underlying mechanism of the disease pathology. Additionally, it has generally been accepted that the annoying symptoms of the disease are generated inside the Blood Brain Barrier (BBB). This assumption, which has little evidence supporting it, has been weakened by the recent observation that domperidone, a DA blocking agent that does not cross the BBB, worsens the severity of WED symptoms. In 1974, it was discovered that levodopa dramatically relieves WED symptoms, thus supporting the hypothesis that insufficient dopaminergic function contributes to WED pathogenesis. Earlier, in 1970, it was observed that venous infusion of DA diminishes thyrotropin levels, and from clinical studies, it is known that WED symptoms are worse in the evening and night, when thyrotropin activity increases. Furthermore, drugs that alleviate WED symptoms increase the DA activity or decrease the Thyroid Hormone (TH) activity, whereas drugs that worsen WED tend to have the opposite effects on DA and TH activity. In this article, we present robust evidence to support the hypothesis that WED is caused by an imbalance between DA and TH and that its symptoms are generated in the periphery of the somatosensory system. We theorize that WED should be considered a functional peripheral neuropathy.
Willis-Ekbom disease (WED), also known as restless legs syndrome, is a common sensorimotor disorder characterized by a strong, nearly irresistible urge to move the legs when the patient is at rest [1]. The currently accepted definitions of adult RLS from the “International Restless Syndrome Study Group (IRLSSG)” and the “International Classification of Sleep Disorders, second edition (ICSD- 2)”, are described below (italic). All four features are necessary to make the diagnosis in adults and children [1,2].
1) An urge to move the legs is usually accompanied or caused by uncomfortable paresthesias and/or pain in the legs. When the paresthesias are not present, patients may only state that they are uncomfortable with inactivity, and as such, they have to move the legs. Many of these patients cannot precisely describe this inactivity or discomfort. Put simply, quietness drives the patient to move.
2) The urge to move or unpleasant sensations begin or worsen during periods of rest or inactivity, such as while lying or sitting. The urge to move may not be restricted to the legs but also extends to other parts of the body, mainly the arms.
3) The urge to move or unpleasant sensations are partially or totally relieved by movements such as walking or stretching, as long as the activity continues.
4) The urge to move or unpleasant sensations are worse in the evening or night than during the day or only occur during the evening or at night. This is considered the hard-rock criterion: if one subject has all of the first three criteria but not this fourth one, a WED diagnosis cannot be made, according to IRLSSG.
The main supportive clinical features of WED include a positive family history of WED, Periodic Limb Movements during Sleep (PLMS), and periodic limb movements during wakefulness (PLMW). An additional supportive clinical feature is the “improvement of RLS symptoms with dopamine (DA) therapy” [1-3].
As mentioned above, WED can be described as a sensorimotor disorder. As such, a better understanding of its pathogenesis may be obtained through separate analysis of its sensory and motor components. From clinical experience with WED, it is known that movements are caused by discomfort in the legs when the patient experiences a resting behavior. Movement tends to relieve the discomfort, thus suggesting that movement is a response to the discomfort. Although it is difficult for the patient to deliberately not move, he/she is able to remain still for a variable lapse of time, and additionally, the patient can stop moving when someone orders it. Likewise, the patient is able to move just one leg even when the desire is to move both. From these clinical observations, it is reasonable to suggest that the motor part of the disease most likely is not pathological by itself. Rather, the movements of a person during a typical WED symptom episode are entirely physiological, and they obey the normal mechanisms of movement physiology. Following this reasoning, the outstanding question is what causes the discomfort in WED patients.
Regarding the sensory part of WED clinical presentation, a question must be addressed: Are WED symptoms generated in the periphery of the nervous system, or are they born centrally? [4]. Ekbom, who initiated studies on WED in 1945, was one of the first researchers to describe RLS in amputees (1961) [5,6]. In his paper [7], he hypothesized that the symptoms were generated in the periphery of the nervous system. There is currently no definitive proof of this hypothesis [8]; however, various clinical insights argue that WED symptoms are indeed generated in the periphery of the somatosensory system [9]. Recently, we hypothesized that stimuli of sensory receptors located deep inside the legs spread up to the somatosensory cortex and are felt as unpleasant WED symptoms when not appropriately modulated [9]. Frequently, applying massage or cold pads onto the legs or simply stretching them can relieve WED symptoms [8]. Commonsense reasoning indicates that these measures applied in the periphery would fail to relieve symptoms born centrally [4]. Furthermore, some patients who have had one leg amputated may have WED symptoms only in the missing limb (phantom WED) [7,10]. In addition, some patients who have undergone total knee arthroplasty surgery begin to experience WED symptoms only in the leg that underwent the operation [11]. Thus, many logical arguments suggest that the peripheral somatosensory system initiates WED symptoms. According to normal physiology, the peripheral somatosensory receptors deep inside the legs receive stimuli from the environment and send their signaling to the cortex. Regarding this function in WED sufferers, we have posited (2010) that WED symptoms may result when the threshold of sensory receptors is reduced and/or the strength of the neurotransmission is high enough to surpass the levels that can induce modulation by DA (and other modulation systems) [11,12]. If WED symptoms originated in the brain itself, then they would be hallucinations, which is an inappropriate hypothesis considering the clinical correlates of WED. Models of dopaminergic dysfunction in RLS focus on central dopaminergic neurons, meaning those inside the Blood Brain Barrier (BBB). However, recently it has been observed that domperidone, a peripheral dopamine blocker that cannot cross the BBB, dramatically worsens WED symptoms in Parkinson’s disease patients [13]. This observation strongly challenges the hypothesis that WED symptoms are generated inside the brain. Of the four major neural DA systems, the only one where DA can be counteracted by domperidone is the tuberoinfundibular pathway. The hypothalamus releases DA as a neurohormone in the pituitary stalk, where it mainly functions as an inhibitor of thyrotropin and prolactin hormones.
Recently, we hypothesized that the neurohormone DA, released by the arcuate nucleus of the hypothalamus in the tuberoinfundibular pathway, is not sufficient to inhibit the release of thyrotropin by the thyrotrophs of the pituitary, causing WED symptoms to occur in some subjects. We refer to this as the imbalance between DA and thyroid hormones (TH) theory (IMBDA/TH) on WED pathophysiology [12]. Increased TH levels, secondary to an insufficient modulation of thyrotropin by DA, diminish the threshold for stimuli perception of somatosensory receptors located deep inside the leg and also increase the synaptic velocity of perceived stimuli on their way to the somatosensory cortex, where they are felt as unpleasant sensations [11].
In the 1970s, it was observed that the intravenous infusion of DA decreases thyrotropin levels [14]. DA does not cross the BBB, so its action on thyrotropin levels is exercised outside the BBB and likely in the DA tuberoinfundibular pathway, the most important site where thyrotropin is released. Additionally, it was observed that metoclopramide increases thyrotropin and TH levels [15,16], which is important because metoclopramide worsens the severity of WED symptoms [8]. Domperidone, which does not cross the BBB, acts as a DA blocker and equally worsens WED symptoms. These observations suggest that DA blocking agents worsen WED symptoms by acting in the tuberoinfundibular pathway, thus leading to impaired thyrotropin inhibition.
To summarize, DA diminishes thyrotropin levels (consequently, TH levels are also reduced) [14], and DA agonists mitigate WED symptoms [6]. DA blocking agents in the tuberoinfundibular pathway increase thyrotropin levels by impairing DA actions [14,15] and worsen the severity of WED [6]. Furthermore, elevated TH levels (e.g., Grave’s disease) remarkably increase the incidence of WED symptoms [17,18]. Adding more plausibility to the IMBDA/TH, it is known that WED symptoms appear (or worsen) in the evening and night [6,8], a time when thyrotropin levels are increased compared to daytime levels [19]. Additionally, from clinical practice, it is known that many drugs that worsen WED symptoms increase TH activity by inhibiting the 3A4 isoform of cytochrome P450 where part of TH is degraded (e.g., calcium channel blockers; SSRIs) [8,12]; some drugs that relieve WED symptoms diminish TH activity by inducing the 3A4 isoform of cytochrome P450 (e.g., Saint John’s Wort) [20]. Notably, it has been observed that the tuberoinfundibular and mesolimbic DA pathways in the brain regulate the expression of the cytochrome P450 system of enzymes in rats. Additionally, the DA agonist pramipexole decreases thyrotropin levels as a side effect after just a single oral administration [21-23].
Ultimately, it can be posited that WED is a very mild form of thyrotoxicosis with a circadian presentation, meaning that there is enhanced TH activity in the evening and night. Clinical observations demonstrate that patients in a thyrotoxicosis condition are characterized by nervousness and hyperkinesia. During a medical interview, these patients shift positions frequently and often without purpose. Fidgetiness is a hallmark characteristic of both WED and thyrotoxicosis patients [24] (Figure 1).
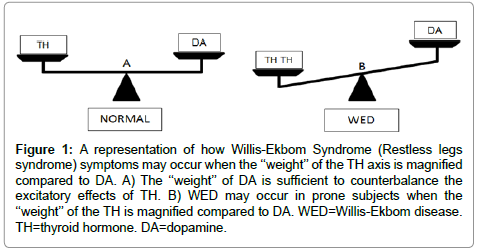
Figure 1: A representation of how Willis-Ekbom Syndrome (Restless legs syndrome) symptoms may occur when the ‘‘weight’’ of the TH axis is magnified compared to DA. A) The ‘‘weight’’ of DA is sufficient to counterbalance the excitatory effects of TH. B) WED may occur in prone subjects when the ‘‘weight’’ of the TH is magnified compared to DA. WED=Willis-Ekbom disease. TH=thyroid hormone. DA=dopamine.
TH affects virtually every organ system in the body, and it is crucial for the normal functioning of our sensory systems [25,26]. TH increases the basal metabolic rate, heat production, and oxygen consumption. It also alters cardiovascular and respiratory function to increase blood flow and oxygen delivery to the tissues. A vast array of proteins is synthesized under the direction of TH, including the NA+- K+ ATPase, the Ca2+ ATPase transport proteins, β-1-adrenergic receptors, lysosomal enzymes, and proteolytic enzymes [26]. Most TH actions are exercised by long-duration, slow-acting genomic effects [26]. Relative to the timescales of our circadian rhythms and to the fluctuation of symptoms of a typical WED patient over the course of a day, the genomic actions of TH are quite slow, which would suggest that these mechanisms do not contribute to WED symptoms [27]. However, the actions of TH on mitochondria [26-29] may play an important role in the generation of WED symptoms and in their circadian aspects. Mitochondria are the organelles responsible for adenosine triphosphate (ATP) production, and TH increases their number and activity [26]. Throughout the nervous system, TH increases the strength and velocity of synaptic transmission [26]. In the CNS, an increase in TH levels enhances cognitive processes, and when levels of TH fall, these processes slow [26]. Burnstock et al. introduced the concept of purinergic neurotransmission, and it is now generally accepted that the multifunctional nucleoside ATP is also a neurotransmitter [30,31]. ATP acts mainly as an excitatory neurotransmitter [30,31] and may be the mechanism by which TH acts on alertness. It is common for WED patients to be in a state of hyper-arousal (increased level of alertness) [8]. We hypothesize that TH enhances synaptic transmission and, thus, causes increased vigilance and more WED symptoms in prone subjects.
Adenosine Triphosphate (ATP) acts as a fast excitatory transmitter in several regions of the Central Nervous System (CNS) [32]. In presynaptic terminals, ATP is accumulated and stored in the synaptic vesicles either alone or with other neurotransmitters (e.g., gammaamino- butyric acid (GABA) or glutamate) [32]. Increasing evidence indicates a widespread role for glutamate as a fast-acting excitatory neurotransmitter at different levels in somatosensory pathways [33]. There is evidence that many different neuroactive substances are involved in the transmission and modulation of somesthetic information in the central nervous system, and additionally, there is evidence that glutamate, an excitatory neurotransmitter, has an important role in the ascending somatosensory pathways [33].
We hypothesize that TH acts on mitochondria to enhance ATP production, and then, ATP enhances transmission of the inputs that travel through the somatosensory pathways and glutamate neurotransmission. In this manner, stimuli received by the somatosensory receptors deep inside the leg are too strongly transmitted to the sensory cortex and are felt as unpleasant WED sensations. In this context, the diminished DA activity of the tuberoinfundibular pathway has a causative role in WED pathophysiology by not being able to sufficiently modulate TH actions on the mitochondria. Recently, it was observed that thalamic glutamate/glutamine activity is increased in WED patients, which increases arousal and shortens sleep [34]. This increased glutamate activity may be interpreted as a dense confluence of inputs that come from the peripheral somatosensory receptors, pass through the relay nuclei of the thalamus, and ultimately get to the somatosensory cortex. From the peripheral receptors, these sensory inputs travel in increased strength (secondary to increased TH activity), being facilitated mainly by glutamate and ATP. Together with paresthesias, pain is common in many WED patients [6]. Glutamate may be involved as a neurotransmitter, and most likely, the neuropeptide substance P plays a role [26].
The GABAergic system is the predominant inhibitory system in the CNS [26], and if a drug has the ability to enhance GABA signaling, it may alleviate WED symptoms. Drugs with this profile include the benzodiazepines, benzodiazepine-like drugs, and carbamazepine. Drugs that inhibit the excitability of the sensory neurons that convey messages to the cortex include many anticonvulsant drugs, such as gabapentin, an analog of GABA that is a highly efficient drug for ameliorating WED symptoms [35]. The pharmacological and therapeutic evidence highlight the importance of a strengthened neurotransmission of sensory inputs to the sensory cortex as the ultimate trigger of WED symptoms.
WED is more common or symptoms are more severe in iron deficient patients, and symptoms ameliorate when iron treatment is administered [6,8]. These facts imply that iron plays a central role in WED pathophysiology. These clinical and therapeutic observations may also be explained in terms of the IMBTH/DA as the main cause of WED [20].
Iron is a cofactor of many enzymatic systems [26], and it is reasonable to assume that when it is lacking in the enzymes of which it is part, these enzymes will experience a reduction in their activity, with the intensity correlating with the severity is the iron deficiency [20]. In the chain of reactions ending in the synthesis of DA, iron acts as a cofactor of the enzyme tyrosine hydroxylase (Thy) that catalyzes the conversion of tyrosine into L-DOPA. This step is the rate limiting stage in the synthesis of DA [36]; as such, we suggest that iron deficiency may result in less DA production. Additionally, iron is an integral part of all cytochromes [26], one of them being CYP450, which has a critical role in the degradation of TH (Figure 2).
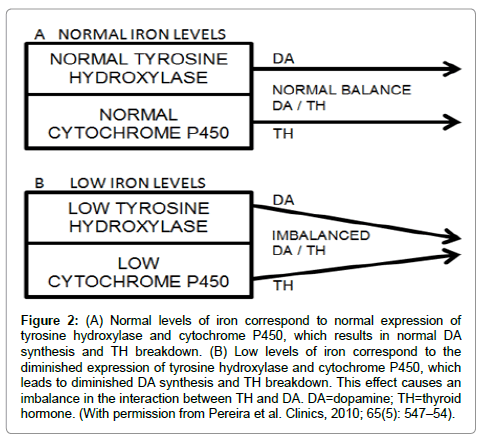
Figure 2: (A) Normal levels of iron correspond to normal expression of tyrosine hydroxylase and cytochrome P450, which results in normal DA synthesis and TH breakdown. (B) Low levels of iron correspond to the diminished expression of tyrosine hydroxylase and cytochrome P450, which leads to diminished DA synthesis and TH breakdown. This effect causes an imbalance in the interaction between TH and DA. DA=dopamine; TH=thyroid hormone. (With permission from Pereira et al. Clinics, 2010; 65(5): 547–54).
As such, it is reasonable to assume that the lack of iron will impair the balance between TH and DA in two ways: (1) by decreasing DA synthesis and (2) by diminishing TH metabolism [20]. Many MRI and ultrasound observations have documented decreased brain iron in the substantia nigra [37]; however, it may be misleading to suggest that the DA dysfunction that causes WED exists in the dopaminergic system of the substantia nigra. It is reasonable to hypothesize that brain iron is scarce because some derangement impairs the brain’s ability to acquire all of the iron it needs, but this is not clear evidence that deficient brain iron causes WED. If the overall levels of iron are deficient, then this deficiency will be observed ubiquitously throughout the brain. More importantly, the levels of ferritin (which is a measure of iron deposits) are low in some WED patients, and when these patients are treated with iron to increase their ferritin levels, they experience an improvement of their WED symptoms [6]. As it is improbable that the WED symptoms are generated inside the brain, it becomes unimportant to know if the brain iron is scarce or not. As iron is a cofactor for THy, iron scarcity may cause impaired synthesis of DA by low activity of the THy.
As dopaminergic agonists alleviate the symptoms of WED, it is more likely that DA hypo function rather than DA dysfunction is the underlying cause of WED. A circadian insufficiency of DA is central to WED pathophysiology. The most significant DA system involved in WED pathophysiology is the tuberoinfundibular pathway, as mentioned above. Synthesized in the dopaminergic arcuate nucleus of the hypothalamus, DA reaches the pituitary portal blood supply. The half-life of DA is extremely short (2 minutes); thus, a dynamic iron supply is required for its synthesis so this trace element may quickly get connected to Thy and boost this enzyme that is so vital to DA production. The blood that bathes the arcuate nucleus is the more logical logistic mechanism to deliver iron for these DA neurons. If there is insufficient circulating iron to be delivered for the arcuate nucleus, the synthesis of DA may be delayed, and then, WED symptoms may ensue in prone subjects. From all this reasoning, it is possible to assert that the iron deficiency theory for WED pathophysiology is ultimately the DA hypo function theory. Recently, it was observed that there is increased THy activity in both WED autopsy and the rodent irondeprivation model of WED, suggesting an increased DA synthesis in WED [38]. Our interpretation for this finding is that the increased presence of THy does not mean increased DA synthesis, as one cannot be certain that this is entirely functional. Iron is a cofactor for the THy protein, and thus if there is insufficient iron to be aggregated and to saturate the parent protein, then this enzyme will not be entirely functional. For DA metabolic production, this means that the enzyme is inappropriately produced and more parent enzymatic protein will be produced, although this excess of enzyme, lacking the cofactor iron, will not be entirely functional. For WED patients who do not have iron deficiency, the cause of the tuberoinfundibular DA hypo production is unknown. Primary WED is most frequently an inherited condition, and the inheritance of impaired enzymatic systems is a common cause of disease in humans, so it is reasonable to suggest that primary WED is a disease caused by some impairment in the enzymes involved in DA synthesis. Additionally, it is possible to speculate that primary WED patients are born with less DA neurons in the arcuate nucleus of the hypothalamus than normal individuals.
From the diencephalic dopamine A11 cell group, in the hypothalamus, dopaminergic neuron projections descend to the spinal cord and primarily reach the dorsal horns at all spinal levels and the associated parts of the intermediate and central gray matter [39]. There is evidence that favors the participation of the spinal dopaminergic system in pain modulation and autonomic and motor responses [40]. The dysfunction of spinal dopaminergic neurons could be involved in the pathophysiology of certain conditions, such as Parkinson’s disease [40]. It appears possible that some beneficial effects of dopamine agonists in this condition as well as some of the side effects of neuroleptics are mediated through their actions on spinal dopaminergic mechanisms [40]. It has been hypothesized (2006) that the diminished activity of this dopaminergic tract is involved in WED pathophysiology [41]. This hypothesis seems well founded. From the somatosensory receptors in the legs, the inputs of unpleasant sensations reach the dorsal horn first and then ascend to the sensory cortex. Inhibitory systems in the dorsal horn modulate the excessive signaling of these sensory receptors to the cortex, which mainly include the GABA system and the mentioned DA system. Pain is common in WED patients, and as this diencephalonspinal DA system is a pain modulator [40], it is likely that this system contributes to the pain and dysesthesia felt by WED sufferers when weakened [41]. In such a situation, dopaminergic modulation on the strong inputs from sensory receptors to the cortex would be diminished. As it is the DA neurotransmitter that plays a role in this mentioned tract, it is likely that DA hypo function underlies WED pathophysiology; DA, both as a neurohormone and neurotransmitter, acts on the hypothalamus to contribute to WED pathophysiology.
Many drugs influence the severity of WED symptoms; some drugs alleviate, whereas others aggravate them. A study of pharmacological profiles suggests that drugs that alleviate WED tend to reduce TH activity, whereas drugs that aggravate WED tend to augment TH. One of these effects may actually be secondary to the diverse actions these drugs have on the Cytochrome P450 system (CYP450): the first induces the system (e.g., dopamine agonists), and the second inhibits it (e.g., SSRIs) [20].
Sequential deiodination degrades approximately 80% of the circulating pool of TH, and the remainder is mainly metabolized within the cytochrome P450 system, where TH is conjugated with glucuronides and sulfates. Glucuronides are then excreted into bile, where they participate as intermediates in the enterohepatic cycle and fecal excretion of TH [42]. Sulfation accelerates the deiodination of different iodothyronines by type I deiodinase and thus initiates the irreversible degradation of the hormone [20,42]. This second pathway is less prevalent and represents approximately 20% of the total TH metabolism [43]; however, for the pathophysiology of WED, it is of great significance. TH behaves similarly to a steroid hormone, and most steroid hormones are substrates for the CYP3A4 enzyme isoform [43]. There is strong evidence that when the CYP3A4 isoform is induced, TH glucuronidation and sulfation are also induced [20,43-45]. Notably, many drugs that relieve or worsen WED symptoms are inducers or inhibitors, respectively, of the CYP3A4 isoform (Table 1). Pramipexole is an effective treatment for WED that is a typical DA agonist with selective affinity for the D2 receptor subfamily [23,46]. Pramipexole also regulates the expression of many CYP450 enzymes through the tuberoinfundibular and mesolimbic dopaminergic pathways [22]. By inducing CYP4503A4 isoform, pramipexole increases TH metabolism. Furthermore, pramipexole administration decreases the release of TSH [47]. These two pharmacological actions of pramipexole may explain why it is effective as a WED treatment. Xenobiotic drugs may also aggravate WED symptoms through decreased dopaminergic signaling [8,20] (Table 1).
| Class of drugs | Examples | CYP3A4 substrates | CYP3A4 inhibitors | Effects on DA system |
|---|---|---|---|---|
| Calcium channel blockers | Verapamil Diltiazem | Yes +++ Yes +++ |
Yes ++ Yes ++ |
No |
| Selective serotonin reuptake inhibitors | Fluoxetine Paroxetine Sertraline Citalopram Escitalopram Fluvoxamine |
Yes + No Yes + Yes +++ Yes +++ No |
Yes + Yes + Yes ++ No No Yes + |
No |
| Neuroleptics | Haloperidol Chlorpromazine Clozapine Pimozide Quetiapine |
Yes +++ Yes + Yes + Yes +++ Yes +++ |
Yes ++ No Yes + Yes + No |
Yes: block DA D2 receptors |
| Anti-nausea agents | Metoclopramide Domperidone |
No Yes + |
No | Yes: block DA D2 receptors |
| Lipid lowering agents | Atorvastatin Lovastatin Simvastatin |
Yes +++ Yes +++ Yes +++ |
Yes + Yes + No |
No |
| Non-steroidal anti-inflammatory drugs | Diclofenac | Yes + | Yes ++ | No |
| Stimulants | Caffeine | Yes + | Yes ++ | No |
Table 1: Suggested mechanisms by which some drugs aggravate WED. The drugs listed in this table (substrates and/or inhibitors of CYP3A4) affect WED by inhibiting the CYP3A4 isoform, thereby decreasing TH metabolism. Some drugs are only substrates of the CYP3A4; nevertheless, they can diminish TH metabolism by competition with TH at sites of the enzyme. In addition, some drugs may cause a direct decline in dopaminergic signaling.
Regarding drugs that improve WED, there are four pharmacological targets for these drugs: 1) diminishing the TSH release (e.g., pramipexole); 2) enhancing theCYP3A expression (e.g., Saint John′s wort); 3) modulating the WED sensation inputs on their pathway from the peripheral sensory receptors to the sensory cortex (e.g., gabapentin); and 4) diminishing the TH release from the thyroid gland by decreasing the SS activity (clonidine) [20]. The beneficial effects of clonidine on RLS symptoms highlight the importance of the connection between the Sympathetic System (SS) and the TH axis. Clonidine, which is an alpha-2 adrenergic receptor agonist, is a sympatholytic agent that relieves WED symptoms in many patients [35]. The SS has nerve projections to the thyroid gland and induces TH release [48] that, when excessive, may cause IMBTH/DA [20]. Clonidine targets the enhanced functioning of the SS, which makes it a useful drug for alleviating WED symptoms that are occasionally generated in response to an exacerbation of the SS tonus [20]. It is known that an enhanced tonus of the sympathetic nervous system impairs sleep [49]. As TH may inhibit sleep [27], we believe that one of the mechanisms by which an elevated sympathetic nervous tonus system hampers sleep is through releasing TH directly from the thyroid gland via its fibers directed to the gland.
Periodic Limb Movements in Sleep (PLMS) consist of stereotypical, intermittent, and repetitive movements of the limbs that occur during sleep [49]. Up to 90% of the WED sufferers present PLMS [49], which is considered to be a supportive criterion for the diagnosis of WED. The concomitance between WED and PLMS is so great that it suggests a common causality between the two conditions, and our assumption is that both are engendered by the same mechanism: increased esthesia of the superficial and deep somatosensory receptors in the legs. The threshold for receiving stimuli from the environment by these receptors is reduced. Stimuli captured by these receptors are transduced and result in exaggerated action potentials and inputs, which strongly reach the spinal cord and then the somatosensory cortex. During wakefulness, these afferent signals prompt a response by the cortex to elicit conscious movements. Our assumption for this movement response is that activity incites a massage effect on the somatosensory receptors. During movement, leg muscles exert continuous and rhythmic pressure on the receptors so that they stop firing to the cortex, similar to what happens when massage is applied to the legs of a WED patient. The patient learns that movements relieve the ailment and movements thus become a conditioned reflex. During wakefulness, four neurons are responsible for the cortex to feel the WED sensation. During wakefulness, the cortex is activated by the reticular activating system, thus it is opened to stimuli that come from the periphery. The patient experiences the typical WED symptoms and consciously responds to them trying to obtain relief. During sleep, the cortex is relatively closed for stimuli that come from the periphery; the sensory cortex does not register WED symptoms. However, the spinal cord does register the inputs coming to it. These sensations are relayed by one of the two axon branches of the pseudo monosynaptic neuron that, located in the dorsal horn, is the neuron responsible by capturing stimuli from the periphery and transducing them into action potentials. As the patient is sleeping, the cortex is closed but the spinal cord is not, and a spinal reflex is triggered: the PLMS. PLMS usually involves the lower extremities, but arms can also be affected. The patient experiences partial flexion of the ankle, knee, and hip with extension of the big toe and fanning of the small toes [49]. PLMS resemble the pathologic slower spinal flexor nocifensive (protective) reflex, the triple flexion reflex. Dorsiflexion of the big toe and fanning of the other toes, found in PLMS, resembles the Babinski sign [50]. It is known that the Babinski sign can sometimes be elicited in normal subjects during sleep [50]. Regarding PLMS, our assumption is that the IMBDA/TH conditions enhance TH activity, which reduces the threshold for stimuli sensitivity of the nociceptors of the somatosensory system. Capturing nonspecific stimuli (allodynia), these receptors fire action potentials that trigger the PLMS, which resembles the triple flexion spinal reflex. Sensory receptors ”adapt” to stimuli and for a variable lapse of time they silence, during which time the patient’s limbs stay still. After this variable lapse of time, receptors recover their transduction capacity and fire action potentials again. As such, as their name implies, the PLMS are observed as periodic nonvolitional movements. Periodic limb movements during wakefulness (PLMW), which some WED patients also present, most likely follow the same triggering mechanisms of PLMS. In our experience, PLMW are usually more prevalent in more severely affected WED patients; their IMBDA/TH most likely is more intense as the PLMW occur even though the wakefulness state is inhibiting spinal reflexes. Recently (2013), it was observed that RLS patients present a 3- to 4-fold increase in sensitivity to pinprick stimuli in both extremities, a sensory pathway involved in withdrawal reflexes [51]. This finding suggests that the somatosensory receptors of WED patients have a diminished threshold for nociceptive stimuli, when compared to normal subjects. This fact adds veracity to the “peripheral- engendered-symptoms” hypothesis, as well as the location where WED symptoms are generated, and also may explain why pain is common in WED patients.
It is noteworthy that not only do many drugs worsen the severity of WED but also many clinical conditions increase the severity of existing WED, or even trigger a new WED episode. For the majority of the medical conditions in this category, there is a recognizable pathology that disrupts the fragile balance between DA and TH through impairing tuberoinfundibular DA release, or inducing an increase in TH levels that surpasses the counteracting capacity of DA in modulating TH actions.
WED during pregnancy is a straightforward example of impairment in DA release. Estradiol levels, mainly during the third trimester of pregnancy, increase considerably with the purpose of inhibiting the release of DA. DA inhibits prolactin, which must be counteracted once prolactin is needed to boost both enlargement of the mammary gland and milk production [9]. Estradiol accomplishes this function and thereby prepares the mother to breast feed the baby. If DA inhibition is too intense, the synthesis of thyrotropin by the pituitary increases too much, leading to WED symptoms [9].
The hyperthyroidism state of Grave’s disease is an example of increased TH levels that surpass the counteracting capacity of DA in inhibiting TH actions, and thus cause WED. In Singapore, a cohort of Grave’s disease patients presented with WED-like symptoms at a prevalence of 8,8% [18]. In Singapore, the prevalence of WED among the normal population is only of 0,9% [17,18]. These numbers support the notion that elevated TH levels can contribute to WED symptoms. However, the fourth diagnostic criterion (worsening of symptoms during evening and night) was not observed in those patients with WED- like symptoms, which precluded the authors from making a definitive WED diagnosis. However, it is known that the increased TH release in Grave’s disease does not follow a circadian rhythm; TH release in Grave’s patients is uniform along the day [52]. As the fourth WED diagnostic criterion is secondary to the circadian production of thyrotropin (increased at evening and night), it cannot be obtained in most Grave’s disease patients with WED-like symptoms. However, in two Grave’s disease patients in this study that previously presented with WED, the symptoms had previously been worse at night, before the onset of the hyperthyroidism. After the hyperthyroidism they started to have symptoms all day, but with worsening of the symptoms in the night.
Many neuropathies may present WED symptoms that fulfill all criteria to diagnosing a definite case, including diabetes neuropathy and some others [6,8]. In the affected patients, damage to their sensitive nervous fibers may expose the somatosensory receptors more overtly to the environment, and thus, stimuli are more intensely captured, transduced, and sent as inputs to the somatosensory cortex, where they will be felt as the annoying sensations of WED. Furthermore, when a denuded (due the neuropathy) nervous fiber is stimulated at any point of its path in the direction toward the cortex, an action potential may be triggered, which will be interpreted by the cortex as coming from the initial site of that fiber location, from the site nourished by that nervous fiber. This principle of labeled lines in the somatosensory system may explain phantom WED in amputees and in patients who have undergone total knee arthroplasty [11]. In this latter situation, the superficial fibular nerve is damaged at its path around the knee, a condition that may trigger action potentials at this site, which will be felt as paresthesias coming from the calf, a region nourished by the superficial fibular nerve. This principle may also explain the phantom limb pain phenomenon experienced by amputees [10,11]. Nerve fibers damaged by a neuropathy disease (not primary WED) may trigger inputs that will be turned into WED symptoms. These inputs follow the same basic transmission mechanisms that govern signals sent to the somatosensory cortex, whether they are conveyed from pathologically hyper sensitized somatosensory receptors or from demyelinated fibers that suffer damage (by the neuropathy) on their way to the cortex. WED symptoms are more common in diabetic patients than in normal subjects [8]. Most likely, neuropathy caused by the diabetic condition underpins the WED symptoms presented by these individuals.
In chronic renal failure, WED is more common than in normal subjects [53]. Most likely, this fact is conditioned by two relatively common complications of chronic kidney failure: 1) uremic neuropathy [54]; and 2) decreased activity of the cytochrome P450 superfamily of enzymes [55,56]. Both conditions are not as yet entirely understood. The first one may reduce the threshold for stimuli of the somatosensory receptors deep in the legs, what causes overwhelming signaling to the sensory cortex. The second may hamper the normal metabolism of TH, thus causing an imbalance between DA and TH.
A better understanding of the players involved in WED pathophysiology may contribute to a better treatment approach for this serious disturbance that affects so many people in the world and that causes much suffering.
The scientific community at large, including physicians of all specializations and health care providers, should be aware of the fragile equilibrium between DA and TH. Endocrinologists should not overlook the importance that DA has as a thyrotropin inhibitor. An appropriate balance between the DA of tuberoinfundibular pathway and the hypothalamus-pituitary-thyroid axis is essential for normal function of one of the most important aspects of our somatosensory system physiology: conveying refined messages from the periphery to the somatosensory cortex.
Primary WED, a sensorimotor disorder, may also be appropriately described as a functional peripheral neuropathy, or an endocrine disease. The first description because the symptoms of the disease are generated in the periphery of the somatosensory system and caused by a hypo function of the tuberoinfundibular dopaminergic system; the second, because the two most significant players in the disease are a classical hormone, and a neurohormone.